Change Language German
Findings
- Typical acute onset of vertical diplopia without ptosis, combined with a characteristic head position
- Head tilt and face rotation towards the healthy side with slight chin lowering
- The affected eye is positioned higher
- Bielschowsky head tilt test: In fourth nerve palsy, the deviation is less when the head is tilted to the opposite side; remember “BOOT = better on opposite tilt”
- If excyclorotation is more than 7 degrees, bilateral trochlear palsy is likely
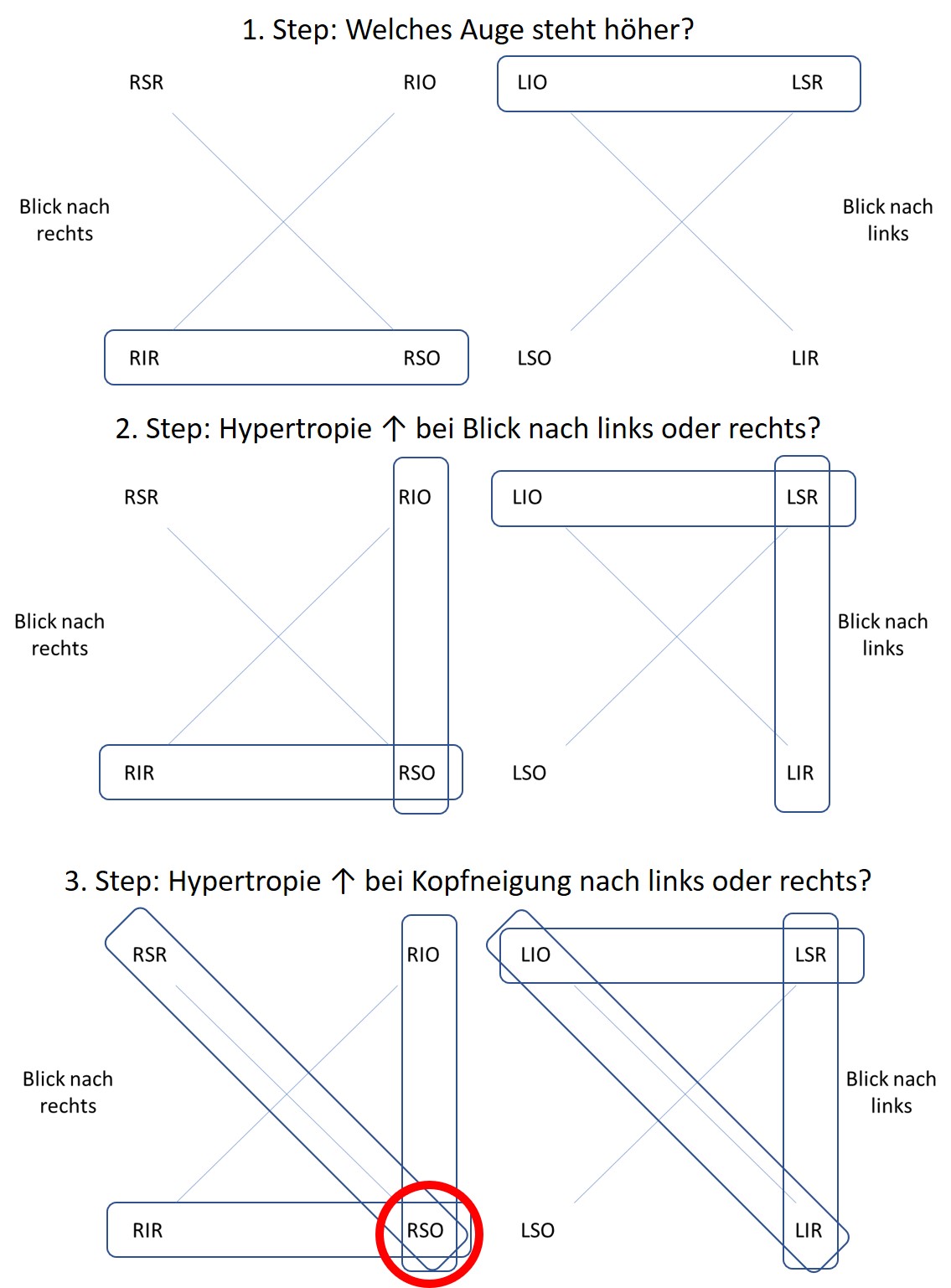
3 Step Test
- Hypertropia due to weakness of an eye muscle: Which muscle is affected?
- Step 1: Which eye is higher in primary position?
- Step 2: Does hypertropia increase when looking left or right?
- Step 3: Does hypertropia increase when tilting the head left or right?
- Example of right trochlear palsy
- Step 4: Double Maddox Rod Test
- Confirmation and measurement of torsion
- Unilateral: typically <10° excyclorotation
- Bilateral: typically >10° excyclorotation
- Step 5: Test in lying and sitting positions
- For suspected skew deviation: Decrease in deviation in the lying position
- Important, as skew deviation is almost never benign: Suspect posterior fossa lesion!
- In trochlear palsy: no difference between lying and sitting positions
- For suspected skew deviation: Decrease in deviation in the lying position
{kind=link}
Bilateral Fourth Nerve Palsy
- In primary position often without visible deviation
- “Reversing” Hypertropia 1: Right eye higher when looking left, left eye higher when looking right
- Double Maddox Rod Test with >10° excyclorotation
- V-Phenomenon-Esotropia: Increase in squinting when looking down!
- Therefore, automatic slight lowering of the chin
- Bilaterally positive Bielschowsky head tilt test
- CAUTION: Difficult to detect, always consider in trauma! Imaging required!
{kind=link}
Causes
- Trauma: Often bilateral
- Vascular lesions (common in diabetes and arterial hypertension)
- Congenital:
- Often first symptoms (intermittent diplopia) when decompensated in adulthood
- typically with high vertical fusion range (>10 prism diopters)
- Look at old photos: Abnormal head posture?
- Idiopathic
- Demyelinating
- Rare: Giant cell arteritis, tumor, hydrocephalus, aneurysms
Approach to isolated fourth nerve palsies
- In patients > 50/60 years with known cardiovascular risk factors:
- Initially, a wait-and-see approach in cases of highly probable microvascular etiology (typically not painful)
- Exclude giant cell arteritis (clinically) -> if suspected: Blood tests (CBC, CRP, ESR)
- Worsening of the condition is possible in the 1st – 2nd week after the event, improvement should follow thereafter
- If the palsy worsens after 6 – 8 weeks -> Plan head MRI (with trochlear palsy, indication for imaging is more generous than with abducens palsies, as it is often not microvascular)
- If no improvement after about 3 months -> Plan head MRI
- In young patients < 50/60 without known cardiovascular risk factors:
- Plan head MRI promptly (within 1 week, not urgently)
- If fourth nerve palsy and herpes zoster ophthalmicus
- Conduct head MRI / MRA including black blood sequences: cerebral vasculitis? (if confirmed, intravenous antiviral therapy is necessary!)
- If fourth nerve palsies in combination with other neurological symptoms or combined cranial nerve palsies
- Urgently refer patients to neurologists for further evaluation
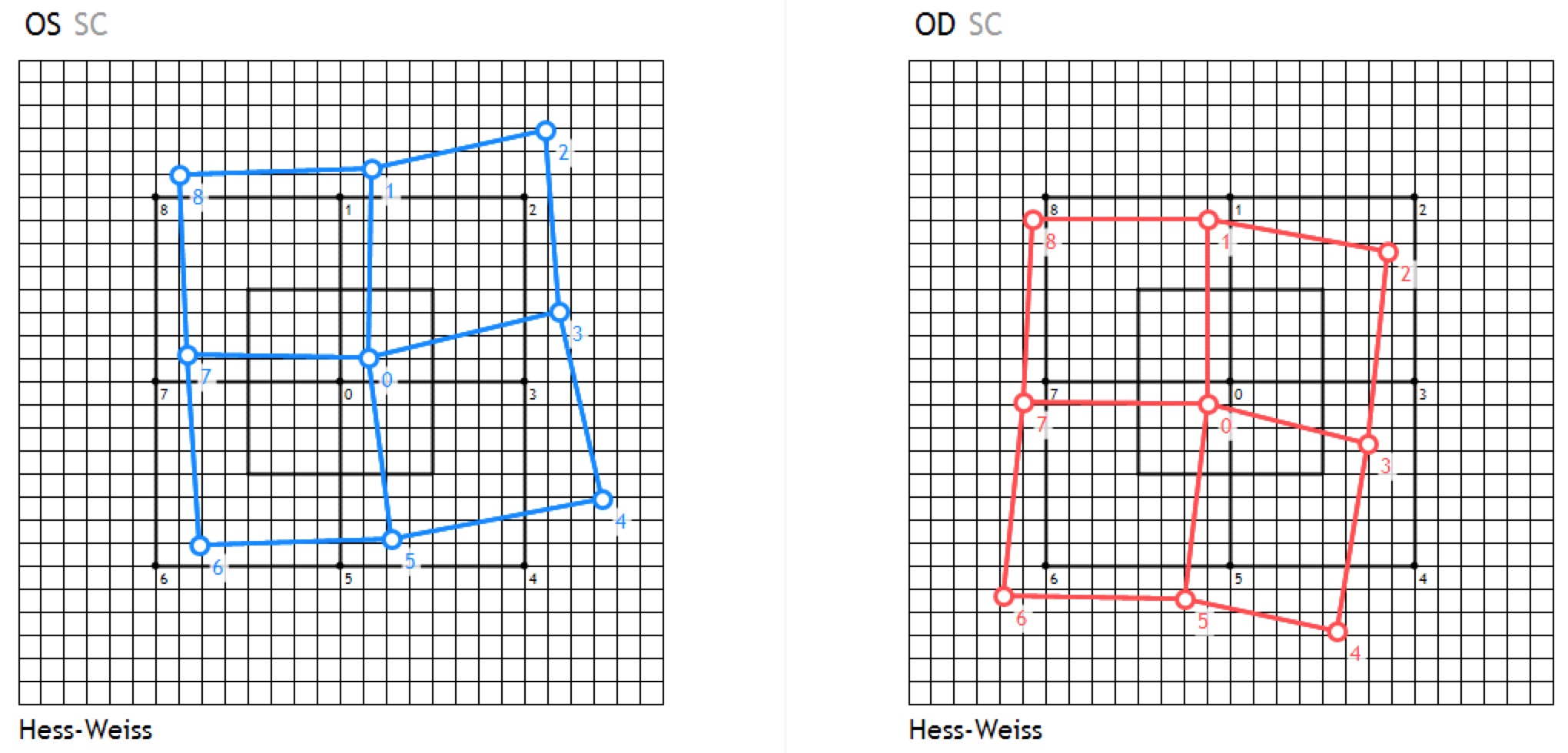
Hess-Weiss-Test / (Harms) Tangent Scale
- Simple, good test providing clues about the type of palsy
- Possible from around the age of 6
- Requires normal binocular vision
- Red markings = right eye
- Blue markings = left eye
- 1 square on Hess-Weiss corresponds to 5 prism diopters and 5° on the tangent scale
- Left Fourth Nerve Palsy
{kind=link}
Sources
- EyeWiki Cranial Nerve IV Palsy
- Trochlear Nerve by Dr. Andrew G. Lee
- Bilateral 4th Nerve Palsy by Dr. Andrew G. Lee
- 3 Step Test by Dr. Andrew G. Lee
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)
- 1 von Eyerounds.org, © The University of Iowa; Licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.
- 1 Contributor: John Chen, MD, PhD; Photographer: Stefani Karakas, CRA