Change Language German
General
- Usually caused by Varicella zoster virus (VZV) or Herpes simplex virus (HSV)
- Often immunocompetent patients (in contrast to Progressive Outer Retinal Necrosis (PORN) in immunosuppressed patients)
Findings
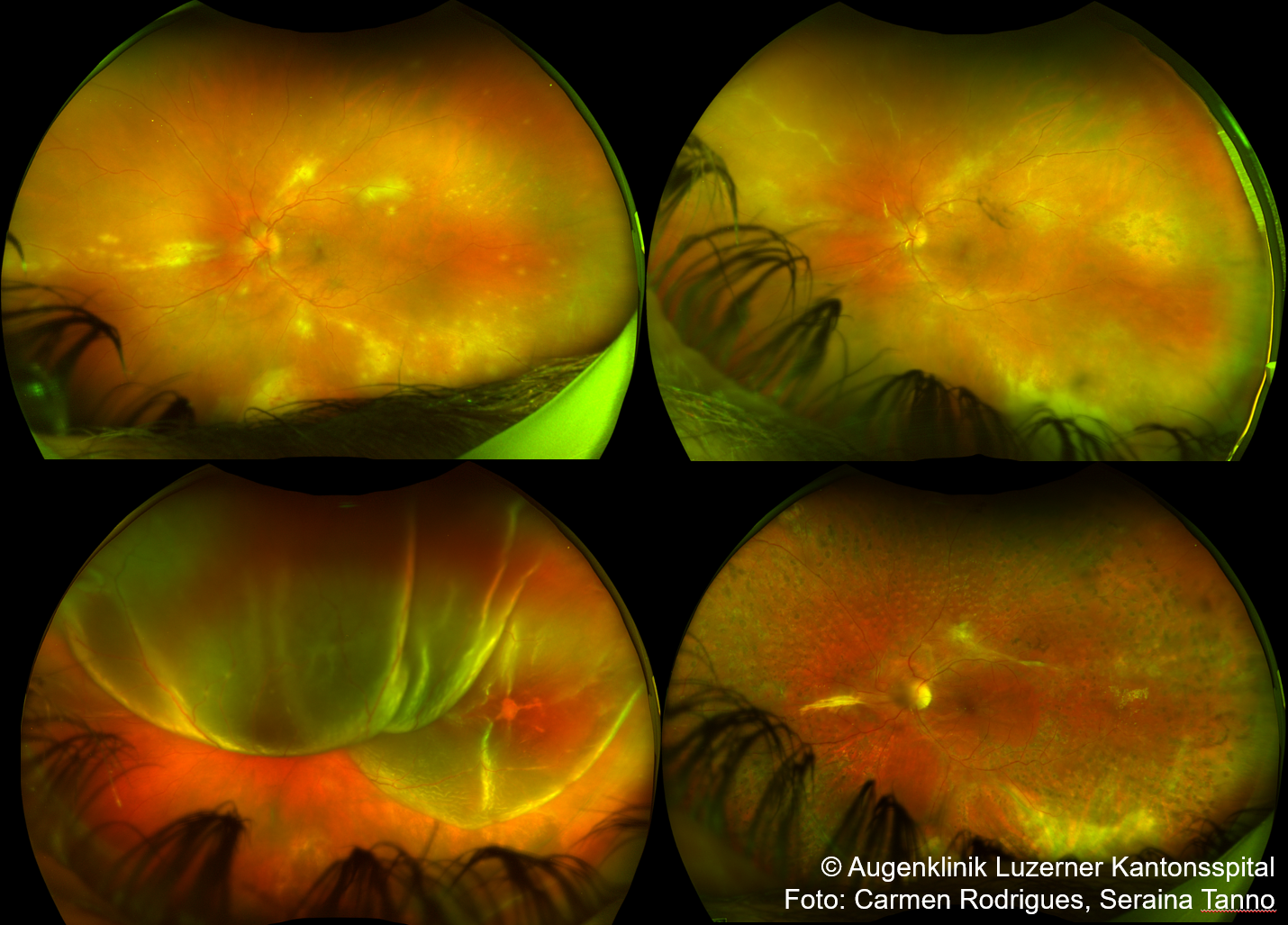
- Retinal periphery with small, multifocal, yellow-white infiltrates, might have haemorrhages
- Rapid progression with circular spread without antiviral therapy
- Occlusive vasculopathy, arterioles affected
- Pronounced vitritis and/or anterior chamber cells
{kind=link}
Diagnosis
- Clinical diagnosis!
- Anterior chamber paracentesis
Follow-up
- Screening (dilated fundoscopy) in patients with Herpes Zoster Ophthalmicus: ocular involvement?
- may occur only after several weeks
- Frequent retinal examinations due to high risk of retinal detachment
{kind=link}
Treatment
- Systemic antiviral therapy with Aciclovir i.v. (10 mg/kg 3x/d for 7-14 days) followed by oral valaciclovir (1000 mg 3x/d) for 3-4 months.
- CAVE: Dose adjustment in renal insufficiency, monitoring of renal values.
- Systemic steroids from day 2: initial dose prednisone 1-2mg/kg
- Consider intravitreal ganciclovir (or foscarnet).
- Consider topical steroids + cycloplegics
- Consider prophylactic laser therapy to prevent rhegmatogenous retinal detachment
Sources
- EyeWiki Acute Retinal Necrosis
- EyeWiki Anterior Chamber Paracentesis in Uveitis
- AWMF Leitlinie – Diagnostik und Therapie des Zoster und der Postzosterneuralgie
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)