Change Language German
Aetiology
- mostly due to adenoviruses (65-90%)
Presentation
- non-specific acute follicular conjunctivitis
- most common
- usually accompanied by mild systemic symptoms such as a sore throat or rhinitis
- pharyngoconjunctival fever
- droplet transmission
- combined with upper respiratory tract infections
- epidemic keratoconjunctivitis
- most severe form, in 80% associated with keratitis
- contagious for 2-3 weeks
Symptoms
- Itching, burning, tearing, foreign body sensation, photophobia
- Initially often unilateral, after a few days bilateral
- History of close contacts (family, friends, acquaintances) with conjunctivitis and any recent viral infections
Findings
- Conjunctival hyperaemia, haemorrhages, chemosis, eyelid oedema
- Conjunctival follicles
- Preauricular lymphadenopathy
- Membranes and pseudomembranes
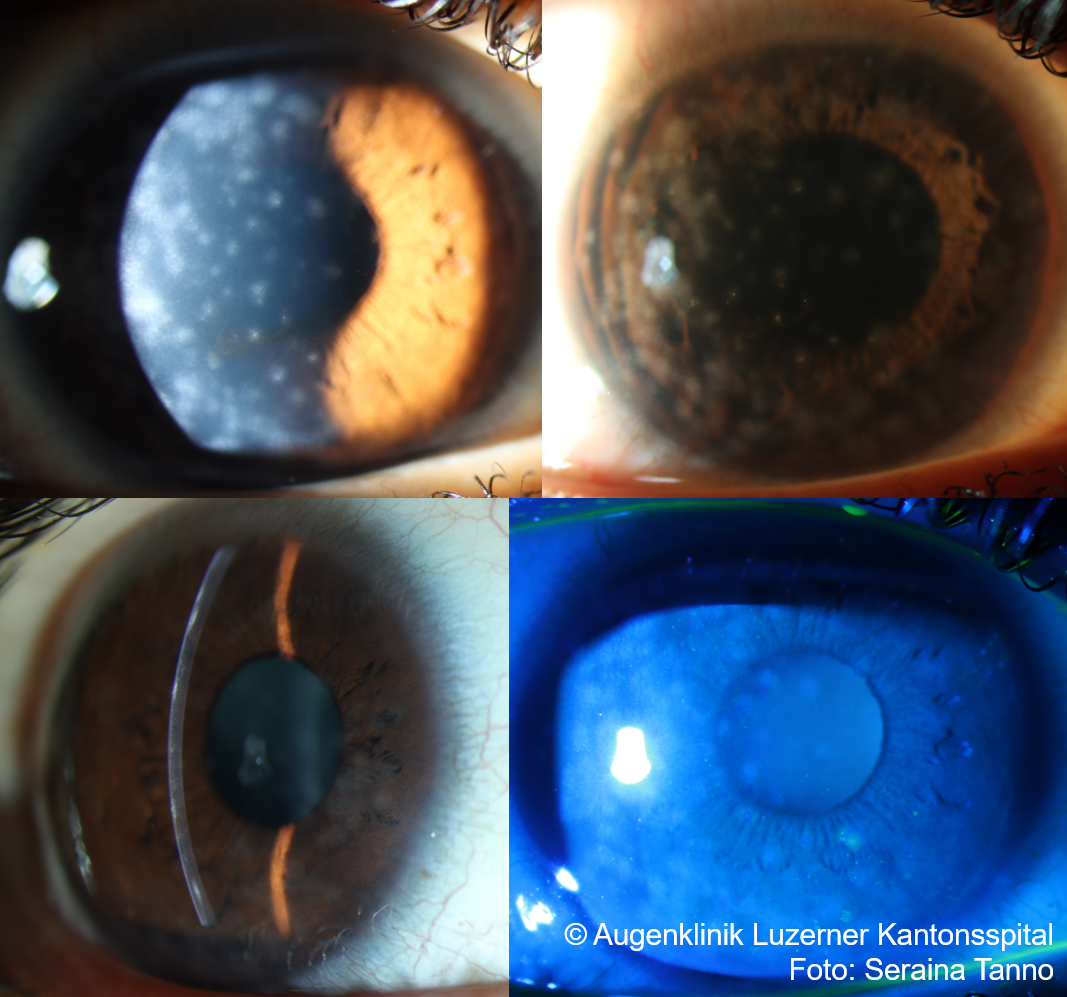
- Epithelial microcysts, epithelial keratitis punctata, subepithelial infiltrates (=nummuli)
- in HSV: vesicles on eyelids or ulcerations of bulbar conjunctiva
{kind=link}
Differential Diagnosis
- Allergic: itching, papillae
- Herpes simplex conjunctivitis: vesicles on eyelids
- Bacterial: more often in children, purulent secretion, hyperacute (gonorrhea, sexual history)
Work-up
- AdenoPlus test (instructional video )
- If possible, do not use oxybuprocaine or other topical anaesthetics because of the risk of a false-positive test, wait at least 5 minutes after the last drop
- Swab the tarsal conjunctiva 6-8 times, then place the swab on one spot for at least 5 sec.
- Hold in buffer solution for 10 sec
- Read result after 10 min
- High clinical suspicion and negative AdenoPlus test: consider taking a swab for adenovirus PCR
- Conjunctival swab for bacteria only indicated if secretion is pronounced or if chronic
Management
- Inform patient about self-limiting course and high contagiousness during first 2 weeks
- Hygiene measures, consider issuing certificate of incapacity for work
- Lacrycon gtt 3-4x daily to hourly
- In case of severe itching, consider antihistamine eyedrops (e.g. Zaditen SDU (Ketotifen) 2x/d)
- See allergic conjunctivitis
- Cooling compresses
- Consider FML NEO gtt (Fluorometholone, Neomycin) 2-3x/d for 5-7 days or Tobradex gtt (Tobramycin) 3x/d for 5-7 days (Cave: steroids are not evidence-based, may increase viral load)
- in epidemic keratoconjunctivitis: Consider Povidone Iodine 0.1% gtt 6x daily for 5-7 days (to reduce viral load)
- If (pseudo)membranes appear: peeling with cotton swabs or tweezers and regular follow-ups
- Consider steroid therapy: e.g. Pred forte gtt (Prednisolone) 4x/d or Ultracortenol ointment (Prednisolone) 4x/d
- In case of subepithelial infiltrates (nummuli)
- good lubrication, usually self-limiting
- in case of severe glare consider therapy with Ciclosporin-A ggt
- Ciclosporin-A 0.1% gtt 1x/day (Ikervis) for 3-6 months
- alternatively Tacrolimus ointment possible
- alternatively Dexafree gtt (Dexamethason) initially 4x/d
- CAVE: frequent recurrences after discontinuation, taper very slowly!
- Chronic infiltrates: Phototherapeutic keratectomy (PTK) for therapy-refractory subepithelial infiltrates with significant visual loss
- CAVE: 10% recurrences
- in Herpes simplex Conjunctivitis
- Virgan eye gel (Gangciclovir) 5x/d
- alternatively Zovirax ointment 5x/d
- Follow-up usually after 2 – 3 days to assess response to therapy
- Virgan eye gel (Gangciclovir) 5x/d
Sources
- EyeWiki Conjunctivitis
- EyeWiki Epidemic Keratoconjunctivitis
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7. Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8. Edition (2015)