Change Language German
Disease
- IgE- and cell-mediated immune reaction
- Bilateral allergic (kerato)conjunctivitis
- Often affects boys in the first decade of life
- 90% have other atopic conditions such as asthma and eczema
- Symptoms most severe in spring and summer
Symptoms
- Redness, itching, tearing
Findings
- Conjunctival hyperemia
- Subtarsal (giant) papillae , sometimes mucus deposits between giant papillae
- Limbal Horner-Trantas dots (elevated gelatinous papillae with white spots)
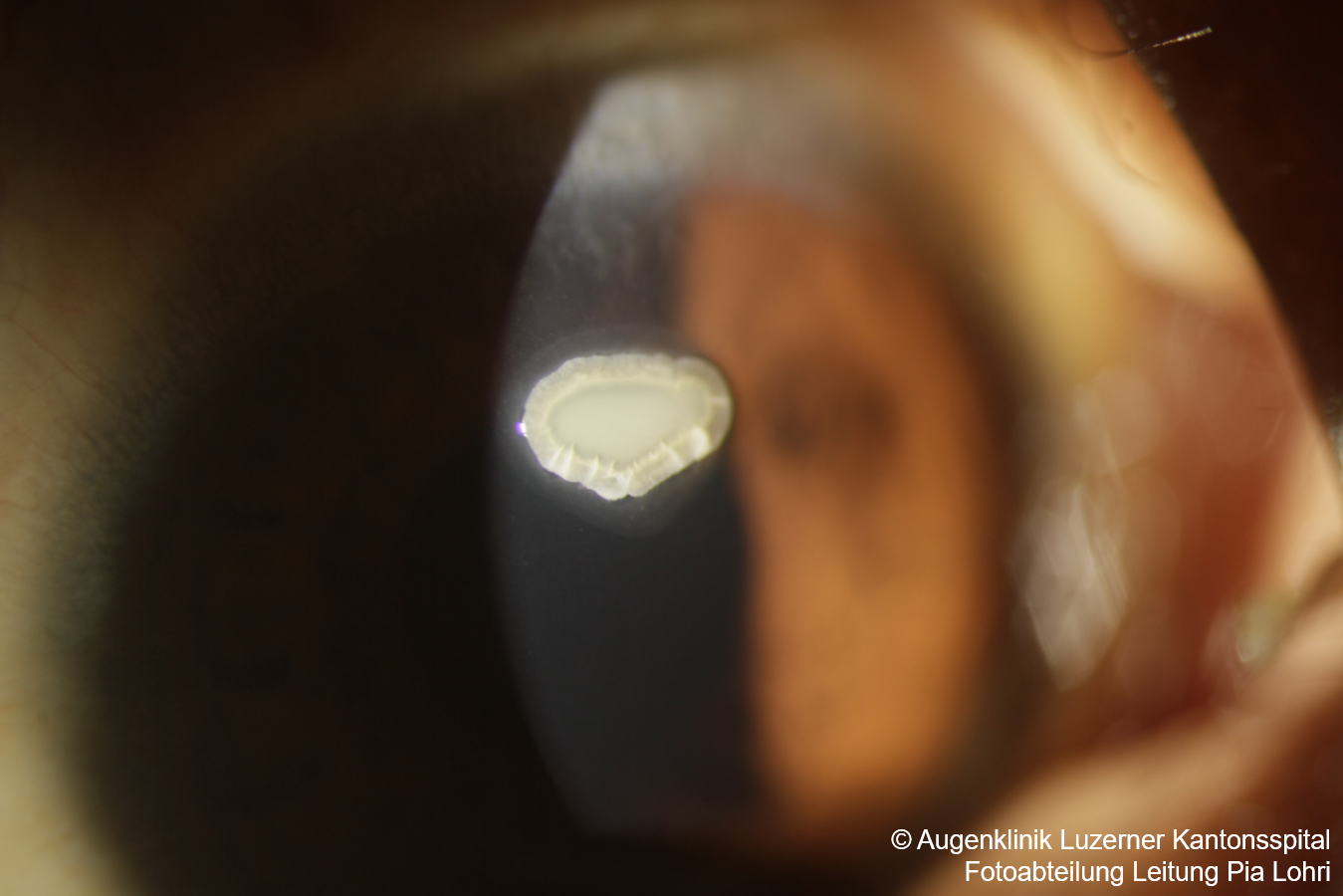
- Corneal shield ulcer (white sterile infiltrate with epithelial defect)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment
- General measures:
- Avoidance of the allergen
- Cold compresses
- Lid hygiene, especially in associated Staphylococcal blepharitis
- Topical medication:
- Mast cell stabilizers, e.g., Cromoglicic acid: Allergo Comod 2% gtt 4x/day
- H1 receptor antagonists, e.g., Emadine SE gtt 4x/day
- Combination preparations, e.g., Zaditen gtt SDU 2x/day or Opatanol gtt 2x/day
- Steroid-containing drops; e.g., Dexafree or FML gtt 3-4x/day, up to every 2 hours in exceptional cases and during acute flare-ups for a few days
- +/- immunomodulators: Cyclosporine 0.05% 2x/day if no response to steroids
- +/- tacrolimus ointment (Protopic) 0.03% 1-2x/day long-term (CAUTION: off-label)
- Consider systemic antihistamines
Differential Diagnoses
Sources
- EyeWiki Vernal Keratoconjunctivitis
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)