Change Language German
Clinical Presentation
- active:
- Solitary inflammatory lesion near an old pigmented scar (“satellite lesion”)
- Ill-defined white lesions with pronounced vitritis (“headlight in fog”)
- White spots along arterioles (Kyrieleis Plaques)
- Possible spill-over with granulomatous anterior uveitis
- inactive:
- Chorioretinal scars at the posterior pole (in the macular region in congenitally acquired disease)
Work-up
- Slit-lamp exam
- Serology: Toxoplasma IgG/IgM
- +/- anterior chamber tap (PCR and Goldmann-Witmer coefficient) in case of unclear clinical presentation
- Imaging in AIDS patients to rule out intracranial toxoplasmosis
Treatment
- Indications for Treatment:
- Lesion near the fovea or optic disc
- Larger or multiple active lesions, pronounced vitritis
- Immunosuppression
- Others: Visual reduction, pregnancy, congenital toxoplasmosis
- Extramacular lesions may be observed without treatment
- Note: No universally accepted treatment regimen!
- “Classic” Therapy
- Pyrimethamine (Daraprim) 100mg/day for the first 2 days, then 25-50mg/day
- Sulfadiazine: Loading dose of 2g, then 4x 1g
- Leucovorin (Folinic acid) 15mg 2x/week
- Alternatives:
- Clindamycin (e.g., 600mg 3x daily); +/- in addition to Sulfadiazine/Pyrimethamine or instead of Pyrimethamine or Sulfadiazine
- Trimethoprim/Sulfamethoxazole (Co-Trimoxazole = Bactrim forte, 160mg/800mg) 2x daily
- Azithromycin (1g on the first day, then 500mg daily)
- Duration of Therapy: at least 4-6 weeks
- Laboratory: Complete blood count, liver and kidney function every 1-2 weeks by general practitioner / clinic
- Steroids:
- In case of threatened vision; Caution: in immunosuppressed patients
- Prednisone initially 0.5-1mg/kg body weight
- Only in conjunction with antimicrobial therapy; consider initiating steroids 24-48h after the start of antimicrobial therapy (controversial)
Prophylaxis
- Bactrim Forte 3x/week for at least 1 year, possibly longer (e.g., in immunosuppression)
Congenital Toxoplasmosis
- Risk of transplacental infection increases during pregnancy; severity of congenital infection decreases over the course of pregnancy
- Retinochoroiditis in >75%
- Fundus examination perinatally with maternal seroconversion, then
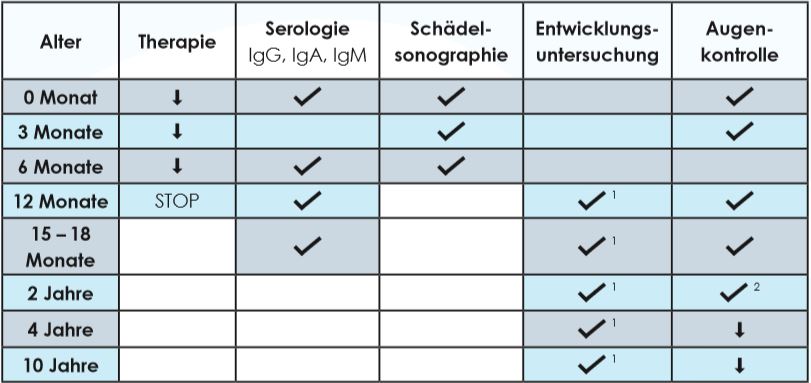
- In asymptomatic infection (serology, no clinical symptoms):
- Fundus examination after 3 and 12 months, then annually until the age of 10
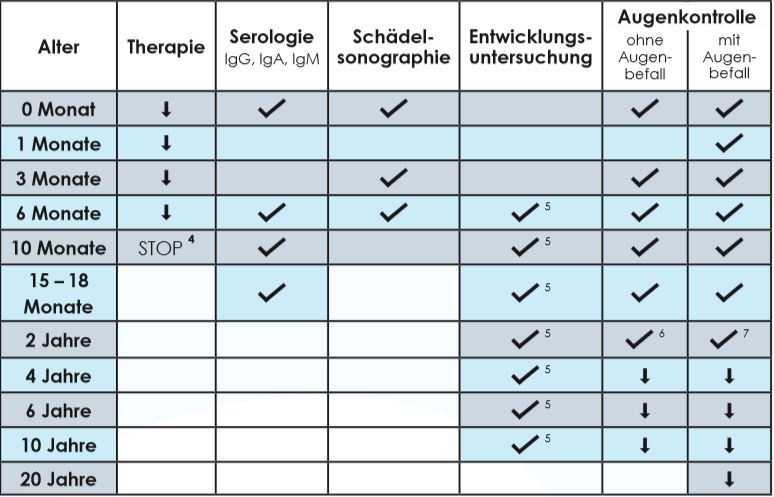
- In symptomatic congenital toxoplasmosis :
- Fundus examination after (1), 3, 6, 10, 15-18, and 24 months, then annually until the age of 10 (without eye involvement) or 20 years (with eye involvement)
- In asymptomatic infection (serology, no clinical symptoms):
{kind=link}
{kind=link}
Sources
- EyeWiki Toxoplasmosis
- Empfehlungen Kongenitale Toxoplasmose, Prof. Dr. J.Garweg, Berner Augenklinik am Lindenhofspital
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)