Change Language German
Clinical Findings
- Severe headaches typically associated with ruptured aneurysm
- Note: Pain may also occur in microangiopathic lesions!
- Double vision
- Ptosis (complete or partial)
- Is the pupil dilated? Poor pupil reaction?
- Deviation of the eye to inferior temporal (complete or partial)
- Restricted motility
Most important Causes
- Aneurysm of the posterior communicating artery
- Most dangerous cause, must be ruled out!
- Stroke, tumor, demyelinating diseases
- Giant cell arteritis
- Rare, but consider in older patients with newly developed double vision!
- Can rarely be the only symptom
- Rare, but consider in older patients with newly developed double vision!
Approach
- Isolated third nerve palsy?
- Other cranial nerves (IV, V, VI) affected?
- If yes, consider other locations such as the cavernous sinus, brainstem
- Other cranial nerves (IV, V, VI) affected?
- Emergency CT scan or immediate CT angiography to investigate for subarachnoid haemorrhage due to ruptured aneurysm of the posterior communicating artery
- If immediately possible, alternatively MRI angiography
- If CT/CT angiography negative: MRI angiography to investigate for stroke, tumor, demyelinating disease
- Pupil involvement
- Typical in aneurysms, trauma, uncal herniation
- Atypical in microangiopathic causes (arterial hypertension, diabetes)
- Theoretically, in complete oculomotor nerve palsy without pupil involvement and existing cardiovascular risk factors, imaging is not mandatory, but normally a CT head is still performed
- If no improvement in palsy within 3 months:
- Arrange additional MRI/MRA examination
- In third nerve palsy and herpes zoster ophthalmicus
- Perform MRI/MRA head including black blood sequences to investigate for cerebral vasculitis (if the latter is confirmed, intravenous antiviral therapy is indicated!)
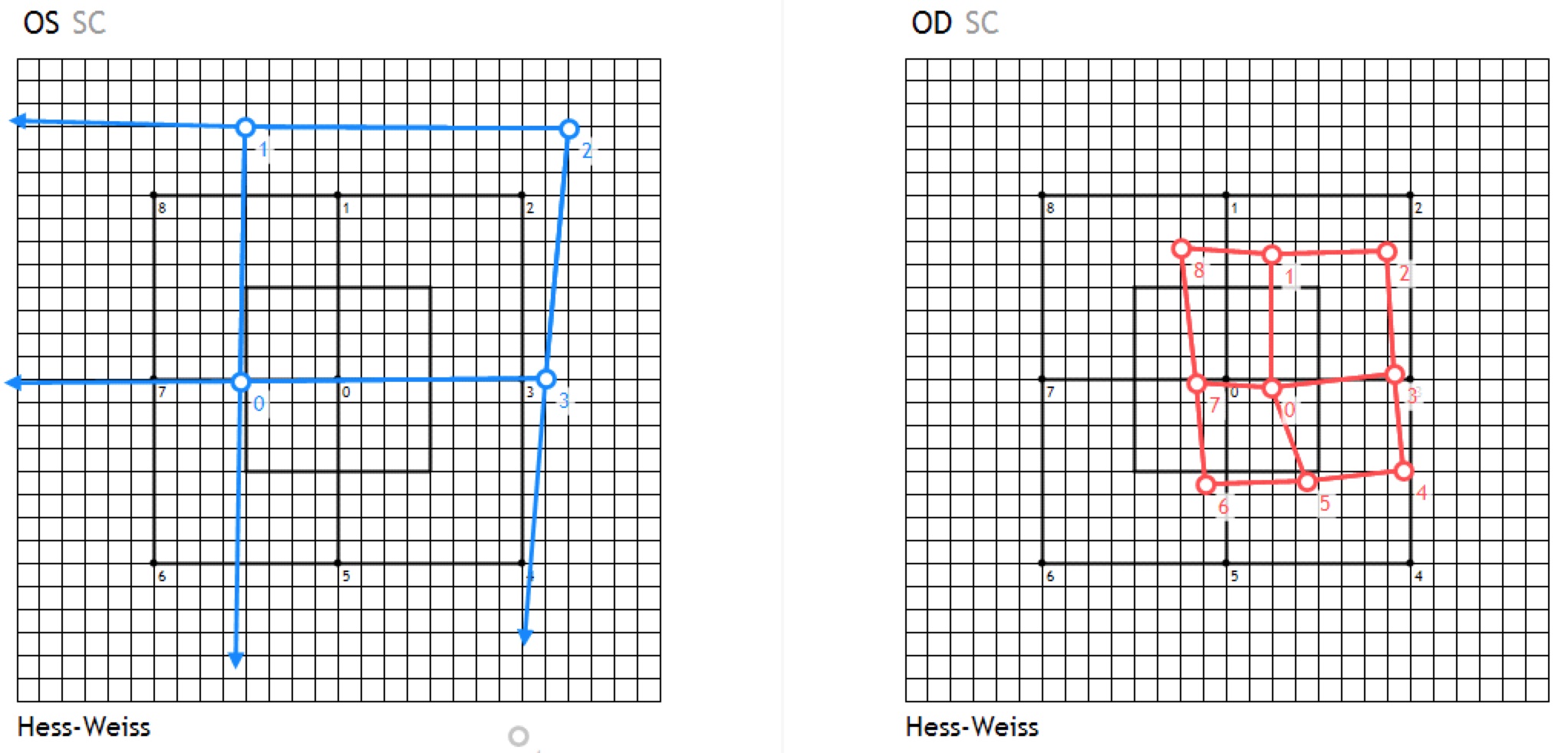
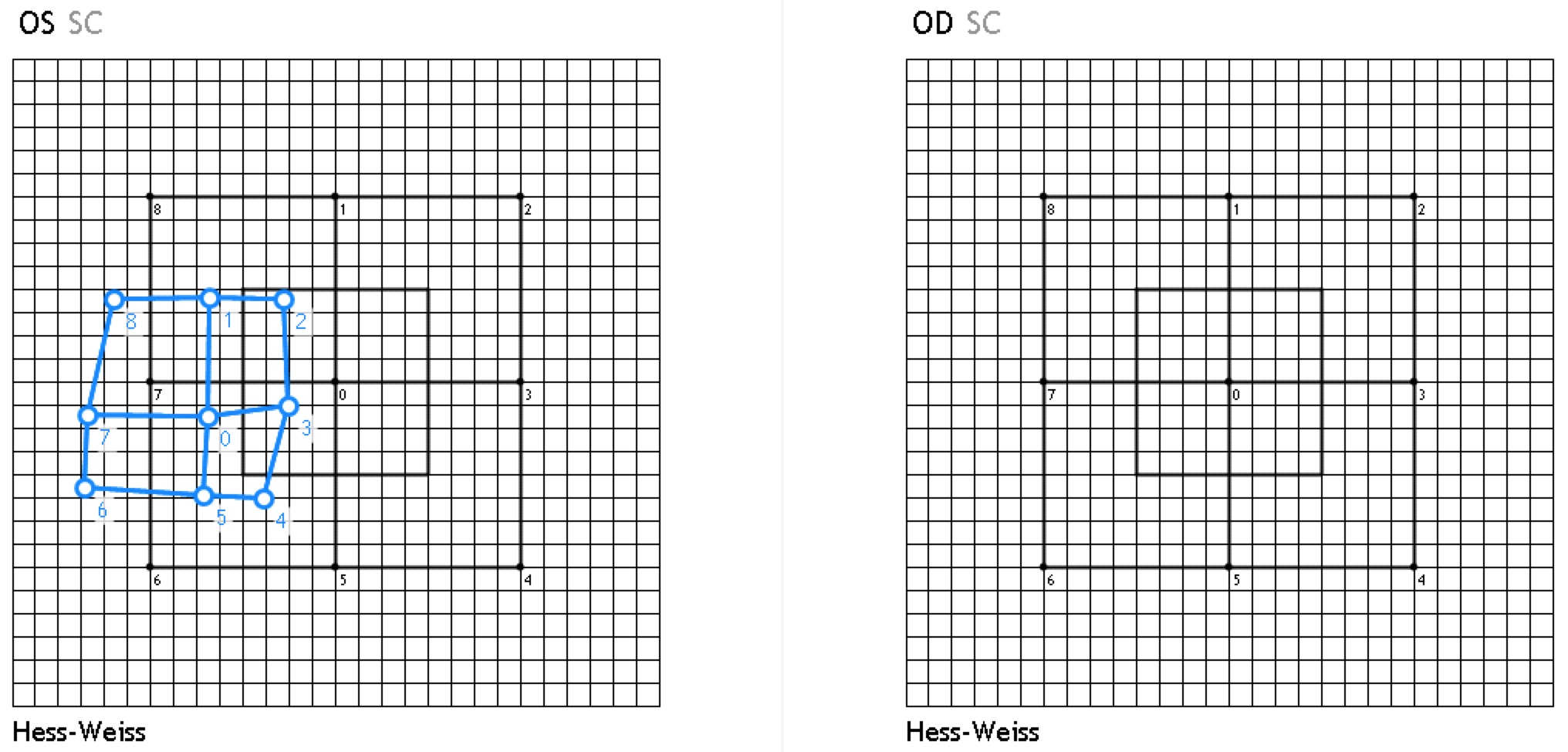
Hess-Weiss/Tangent screen examination
- Simple useful test, indicates type of palsy
- possible from approx. 6 years of age
- A normal binocular vision is required
- Red marks = Right eye
- Blue marks = Left eye
- 1 square on Hess-Weiss corresponds to 5 prism diopters, and 5° on the tangent scale
- Partial oculomotor nerve palsy on the right
- Partial oculomotor nerve palsy on the left
{kind=link}
{kind=link}
Excellent Video by Dr. Andrew G. Lee
Sources
- EyeWiki Acquired Oculomotor Nerve Palsy
- EyeWiki Congenital Third Nerve Palsy
- AAO Third Nerve Palsy
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Kalla Gervasio MD, Travis Peck MD et al; Lippincott Williams&Wilkins; 8th Edition (2021)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; John E Salmon MD; Elsevier; 9th Edition (2019)