Change Language German
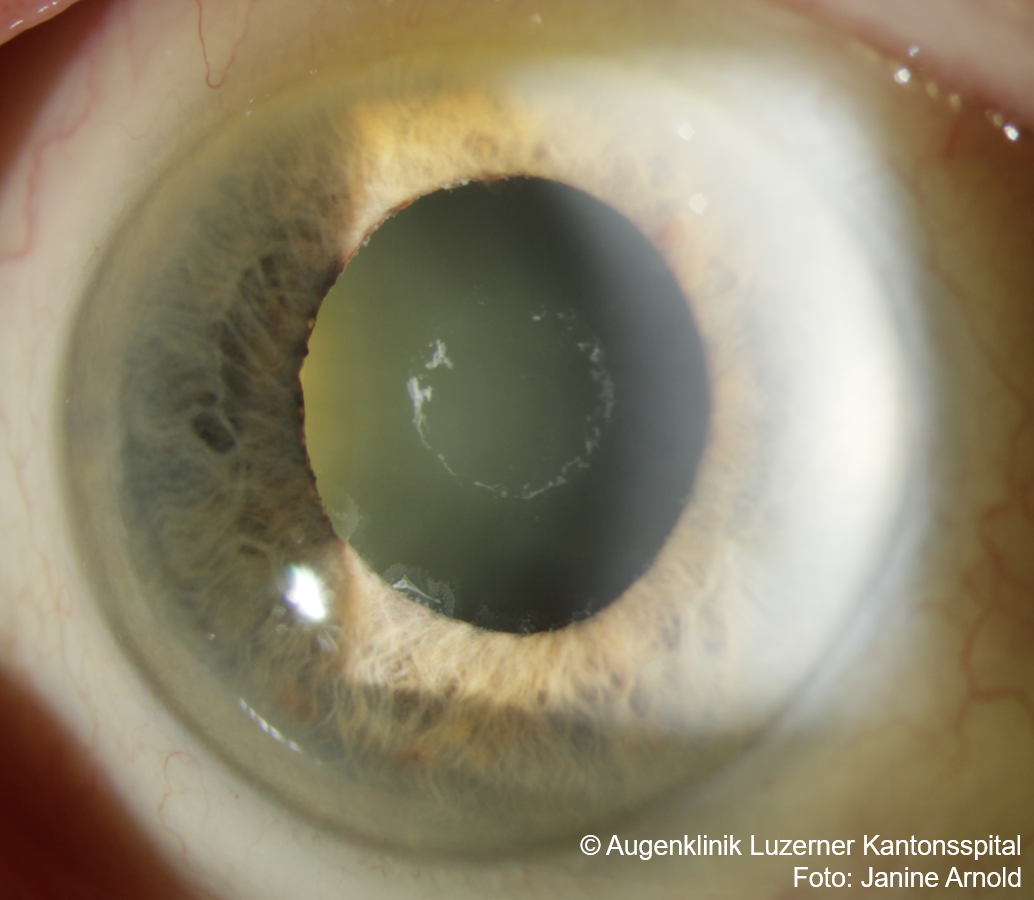
Pseudoexfoliative Glaucoma
- Most common type of secondary open-angle glaucoma
- Usually begins after the age of 60
- Can affect one or both eyes, typically bilateral and asymmetric
- Pseudoexfoliation syndrome if normal IOP and normal optic nerve (regular follow-up to detect transformation into glaucoma!)
- Findings: Pseudoexfoliation material (whitish protein) at the pupillary margin, pupillary margin atrophy, on anterior lens surface
- Gonioscopy: Increased pigmentation of trabecular meshwork (especially inferior), Sampaolesi’s line
- Intraocular pressure (IOP) often higher than in primary open-angle glaucoma (POAG), more diurnal fluctuations
- Often poor dilation, phacodonesis, loose zonular fibers (caution during cataract surgery)
- Treatment similar to POAG, generally responds well to selective laser trabeculoplasty (SLT)
{kind=link}
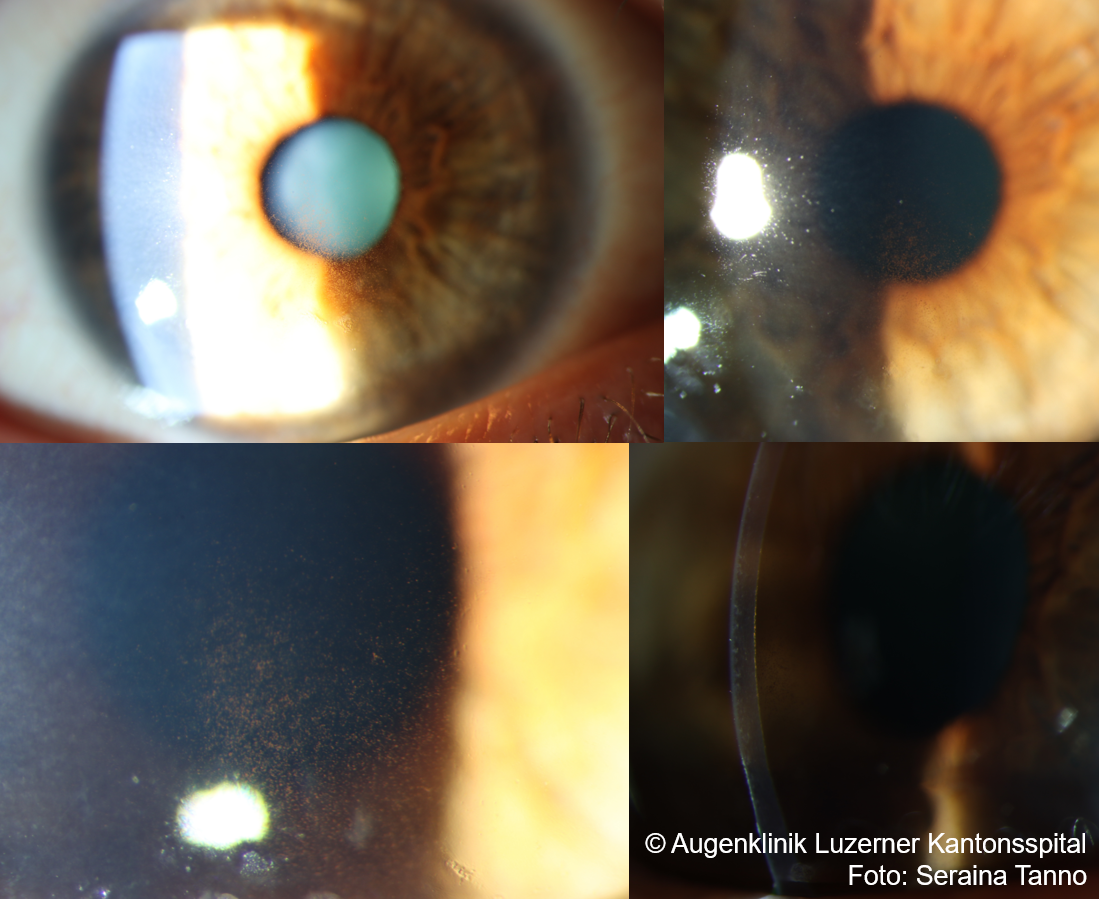
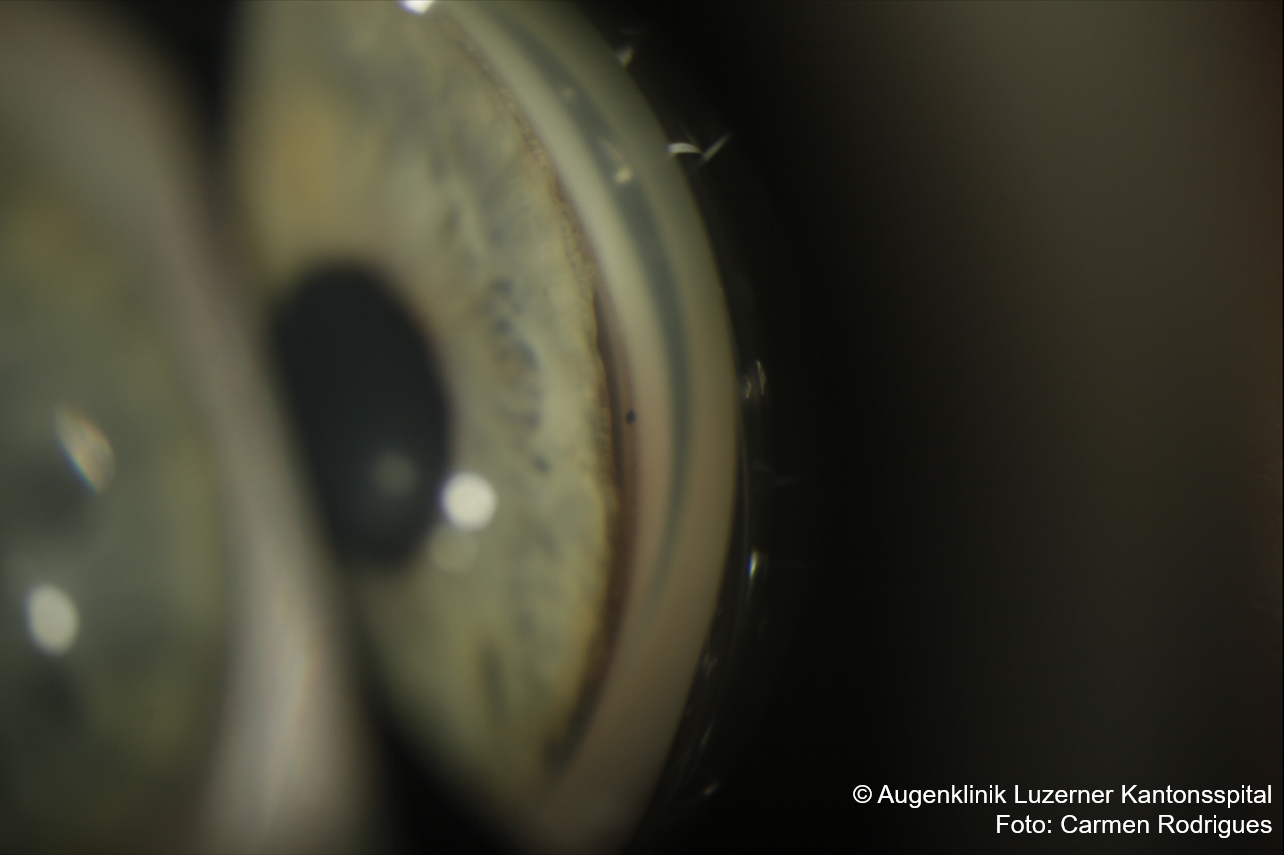
Pigmentary Glaucoma
- Pigment release from the iris pigment epithelium
- More common in Caucasian men with myopia, diagnosis usually around 30-50 years
- Symptoms: sometimes episodes of blurred vision and halos during increased intraocular pressure, often after physical activity or dilated pupils
- Unilateral or bilateral
- Findings: deep anterior chamber with backward bowing of the peripheral iris, mid-peripheral iris transillumination (Krukenberg’s spindle , pigment deposits on endothelium), pigment on anterior lens surface
- Gonioscopy: Heavily pigmented trabecular meshwork, pigment deposition on Schwalbe’s line
- Increased risk for retinal detachment!
- Treatment similar to POAG
{kind=link}
Other Secondary Open Angle Glaucomas:
- Steroid-induced Glaucoma (“Steroid response”)
- Starts about 2-6 weeks after beginning topical steroid therapy
- Discontinue steroids if possible, switch to milder drops (e.g., Lotemax, FML, Softacort).
- Pressure-lowering drops, laser trabeculoplasty (SLT)
- Evaluate glaucoma surgery if high pressure persists
- Lens Induced Glaucoma:
- Phacolytic glaucoma (denatured lens proteins in macrophages clog trabecular meshwork)
- ‘Lens-particle’ glaucoma (lens material post-trauma or cataract surgery clogs trabecular meshwork)
- Phacoanaphylactic glaucoma (lens proteins cause granulomatous uveitis)
- Uveitic Glaucoma (e.g., Posner-Schlossman syndrome, Fuchs uveitis, HSV/VZV, UGH syndrome)
- Glaucoma associated with intraocular hemorrhage:
- Hemorrhagic glaucoma (erythrocytes clog trabecular meshwork)
- Ghost cell glaucoma (old erythrocytes clog trabecular meshwork)
- Glaucoma associated with intraocular tumor (tumor and inflammatory cells clog trabecular meshwork)
- Glaucoma associated with retinal detachment (Schwartz’s syndrome: photoreceptor outer segments likely clog trabecular meshwork in rhegmatogenous retinal detachment; additionally, drainage obstruction due to pigment release from RPE)
- Glaucoma associated with trauma (angle recession )
- Glaucoma due to elevated episcleral venous pressure (e.g., carotid-cavernous sinus fistula, Sturge-Weber syndrome, thyroid eye disease)
{kind=link}
Sources
- European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition,
- Licensed under a Creative Commons License Attribution-NonCommercial 4.0 International CC BY-NC 4.0 DEED
- Eyewiki Pseudoexfoliation Syndrome
- Eyewiki Pigmentary Glaucoma
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Kalla Gervasio MD, Travis Peck MD et al; Lippincott Williams&Wilkins; 8th Edition (2021)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; John E Salmon MD; Elsevier; 9th Edition (2019)