Change Language German
Findings
- Severe eye pain, often at night (sometimes radiating to the forehead, brow, jaw), exacerbated by eye movements and touch
- Acute or gradual onset of redness in the eyes
- Sometimes tearing, photophobia, and visual impairment
Aetiology
- Often (up to 50%) associated with systemic diseases, including:
- Rheumatoid arthritis
- Granulomatosis with polyangiitis
- Recurrent polychondritis
- Polyarteritis nodosa
- Chronic inflammatory bowel diseases
- Less common causes:
- Infectious: Herpes Zoster, Tuberculosis, Leprosy, Syphilis, Lyme disease, Fungi
- Surgically induced: Typically 3 weeks after surgery (strabismus, trabeculectomy, implant, pterygium surgery, etc.)
Forms of immune-mediated scleritis
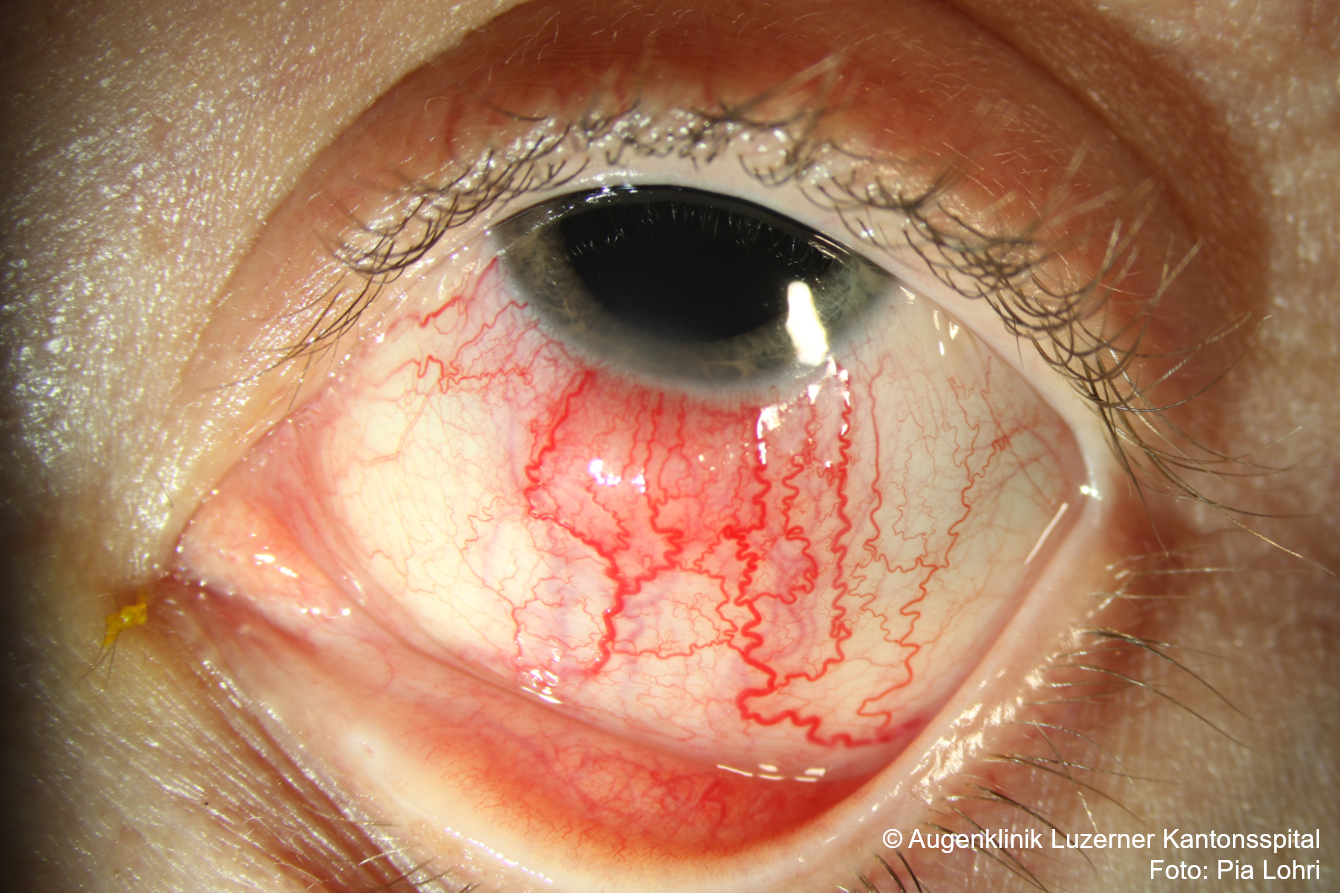
- Anterior Scleritis
- Non-necrotizing anterior scleritis
- Diffuse: Generalised or restricted to one quadrant, with extended scleral, episcleral, and conjunctival vessels
- Nodular: Single or multiple scleral nodules, often in the palpebral fissure, non-movable, intensely dark blue compared to episcleral nodules
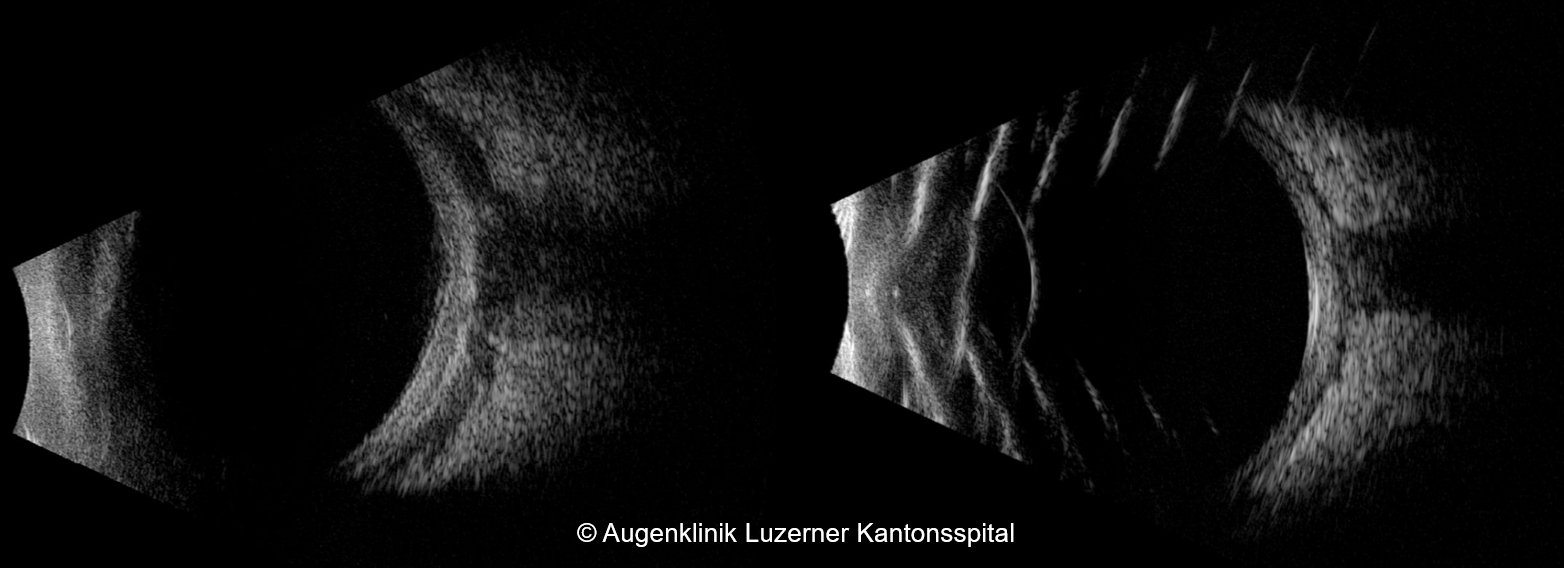
- Anterior Segment OCT
- Necrotizing anterior scleritis with inflammation
- Extreme pain
- Forms:
- Vasoocclusive
- Granulomatous
- Anterior segment angiography, ultrasound biomicroscopy (UBM): Early detection of necrotic areas
- Scleromalacia perforans/necrotizing anterior scleritis without inflammation
- Often asymptomatic/mild symptoms
- Necrotic sclera plaques near the limbus without vascular congestion. Connection and extension of necrotic areas. Rarely perforation.
- Typically in women with rheumatoid arthritis
- Non-necrotizing anterior scleritis
- Posterior Scleritis
- Scleral inflammation posterior to the ora serrata; only 2% of all scleritis cases
- Often associated with anterior scleritis
- Presentation: Choroidal folds, papilledema, macular edema, exudative retinal detachment, uveal effusion, yellow-brown subretinal mass, exophthalmos
- Diagnosis:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Differential Diagnosis
Work-up
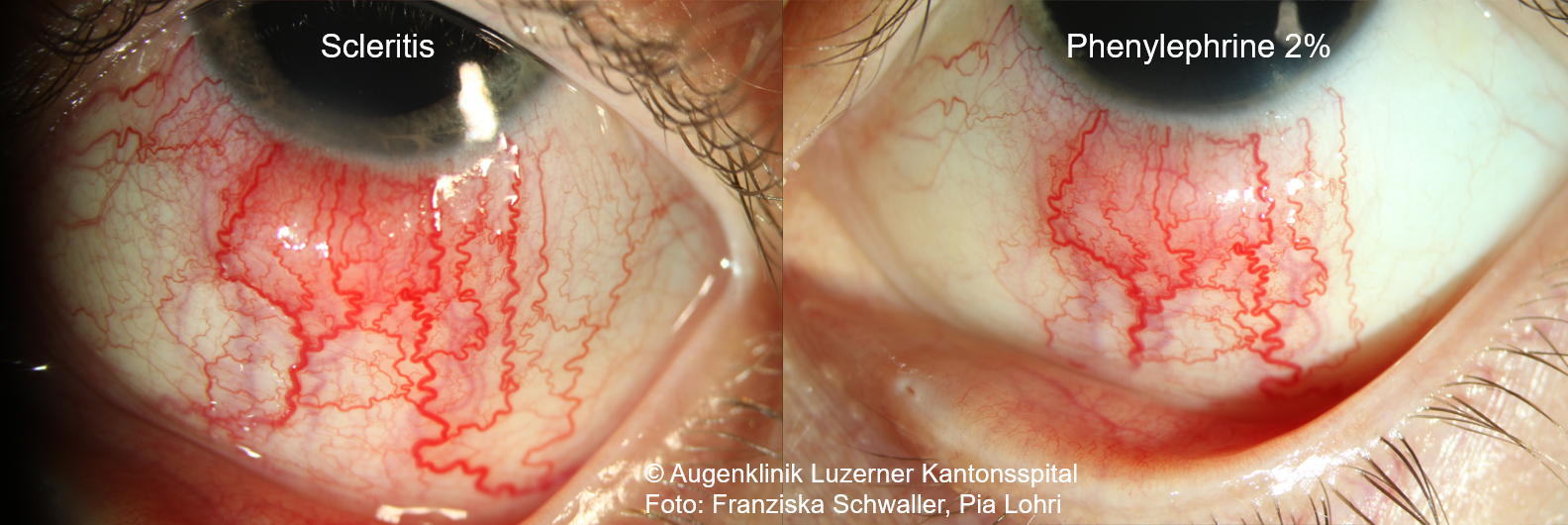
- Phenylephrine test: Administer 1 drop of Phenylephrine 2.5%, evaluate after 10-15min
- if redness persists: Scleritis
- if redness disappears: Episcleritis
- Anterior segment OCT: Helpful for distinguishing between episcleritis and scleritis
- Work-up for systemic diseases recommended
- Differential blood count, ESR, CRP, ANA, ANCA, RF, anti-CCP, ACE, syphilis, , Quantiferon test, chest X-ray
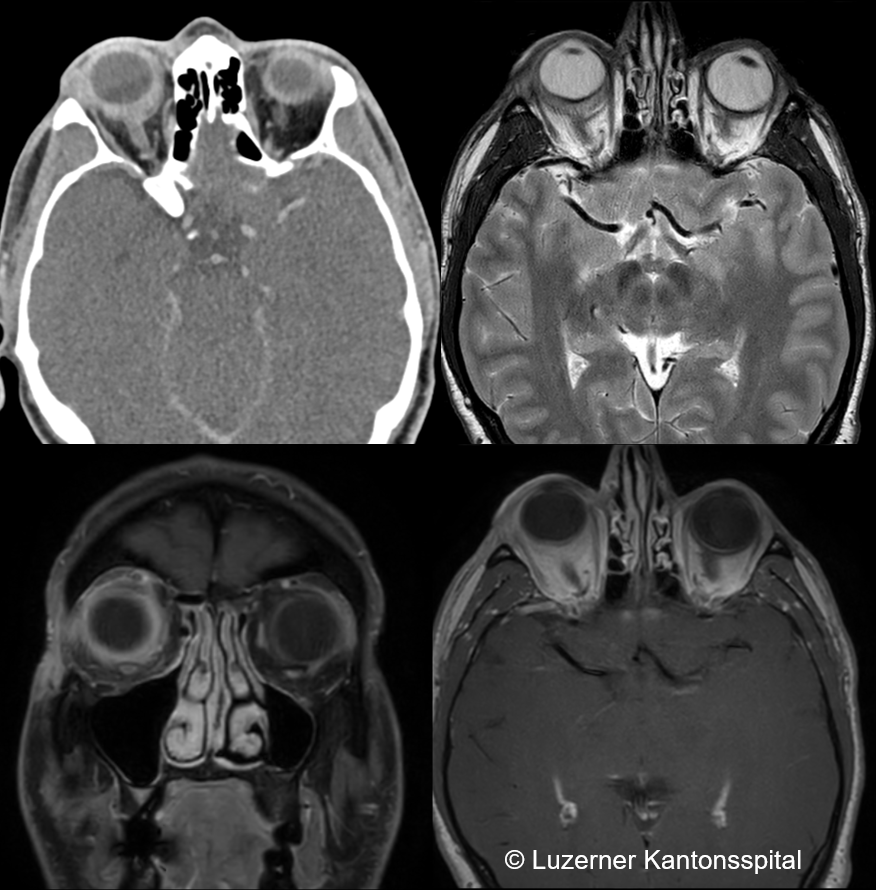
- In case of suspected posterior scleritis: Ultrasound with “T-sign”? MRI/CT: Scleral thickening?
{kind=link}
Therapy for immune-mediated anterior and posterior scleritis
- First choice: Systemic NSAIDs for non-necrotizing disease.
- E.g., Froben (flurbiprofen) 50mg 3x daily or Diclofenac 2×50-75mg for 2 weeks, then 1×50-75mg per day
- Often requires several months of administration
- In case of pronounced findings with severe pain, poor response to NSAIDs, or necrotizing form:
- Systemic steroids: Prednisolone initially 1-1.5mg/kg body weight/day
- CAUTION: Periocular steroid injection is contraindicated in the necrotizing form due to the risk of necrosis!
- CAUTION: In the necrotizing form, in addition to steroids, immediate initiation of immunomodulatory therapy is needed!
- Possible Medications:
- Cytostatics: Cyclophosphamide, Azathioprine, Mycophenolate mofetil, Methotrexate
- Immunomodulators: Ciclosporin, Tacrolimus (mainly used for long-term therapy)
- Specific antibodies: Infliximab, Rituximab, Adalimumab (CAUTION: Rule out tuberculosis!)
- Possibly local steroids for symptom relief (response rate 0-50%), no effect on the course
- Last resort in (threatening) perforation is surgery (then also diagnostic for pathogens)
Sources
- EyeWiki Scleritis
- Tappeiner C, Walscheid K, Heiligenhaus A. Diagnose und Therapie der Episkleritis und Skleritis [Diagnosis and treatment of episcleritis and scleritis]. Ophthalmologe. 2016;113(9):797-810. doi:10.1007/s00347-016-0344-3
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)