Change Language German
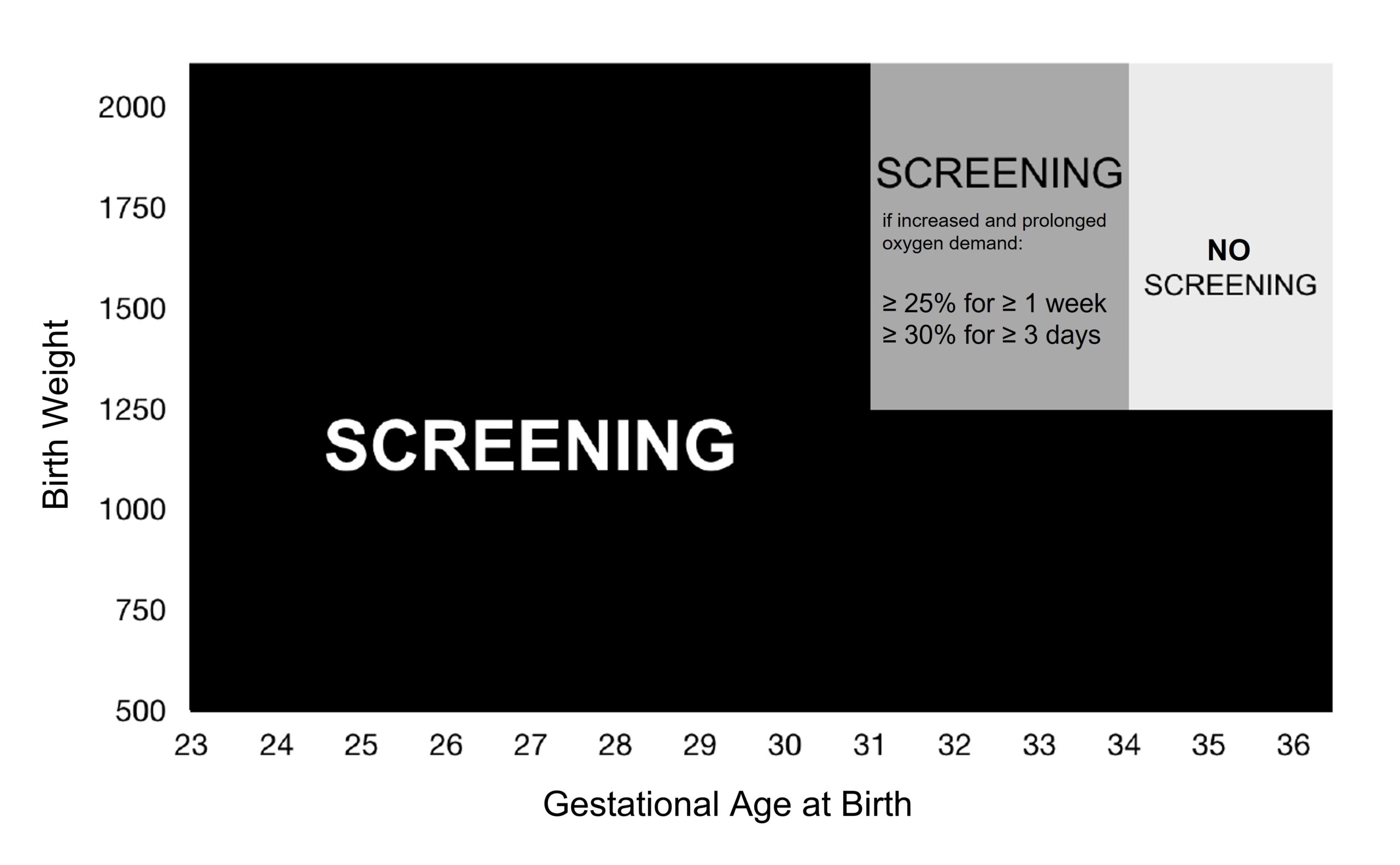
Indication for screening
- Birth < 31+0 weeks or birth weight < 1250g 1
- Premature infants (< 37+0) at risk for ROP development:
- Oxygen therapy of more than 5 days
- Relevant concomitant diseases (e.g. severe necrotising enterocolitis, bronchopulmonary dysplasia, sepsis, anaemia requiring transfusion)
{kind=link}
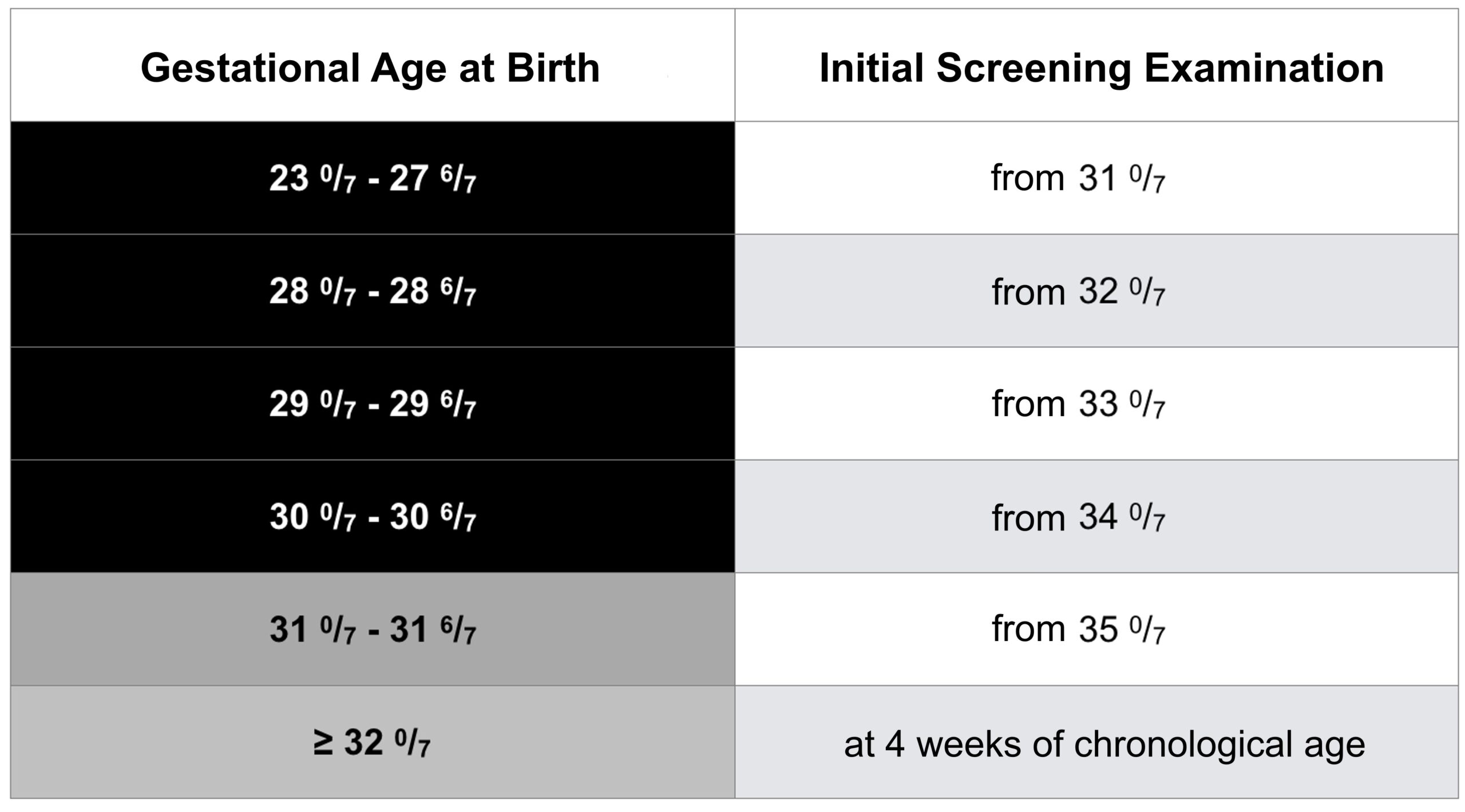
Timing of screening examinations
- Initial screening: 4 weeks after birth but not before 31+0 postmenstrual age 1
- Follow-up examinations
- 2-weekly normally
- weekly or more closely if:
- Vascularisation border in zone I or posterior zone II.
- Vascularisation border in anterior zone II in stage 2 or 3 ROP
- in any ROP with Plus disease
- 3-weekly if vascularisation border in zone III without any ROP
- Extend follow-up intervals by 1 week if
- repeated improved findings
- Calculated date of birth exceeded
- Finish screening of patients without therapy if
- Peripheral retina completely vascularised
- after the calculated date of birth if there is a clear regression of ROP findings
{kind=link}
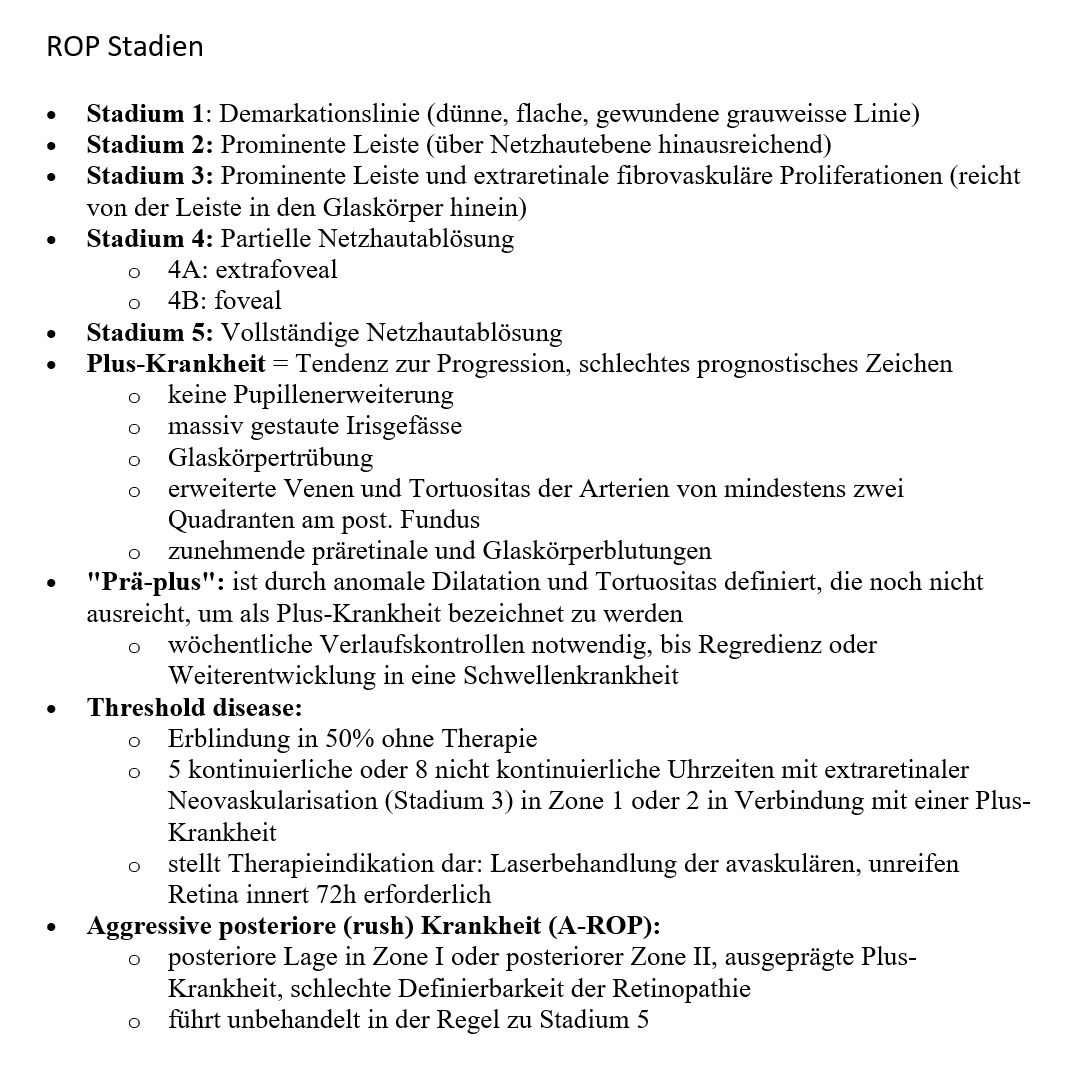
Stages and Zones (ICROP)
- Overview Zones, Stages, Plus Disease, Aggressive ROP (A-ROP) 2,
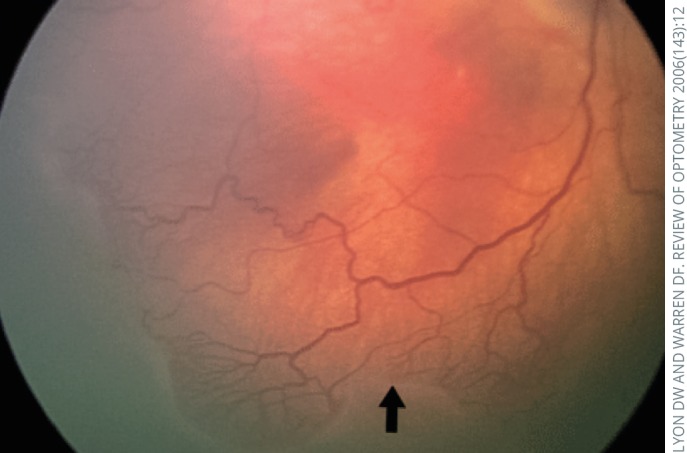
- Stage 1 3: Demarcation line (thin, flat, whitish line between the normally vascularised retina and the avascular peripheral retina).
- Stage 2 3: Visible ridge (with height and widtgh, extending beyond retinal level)
- Stage 3 3: Prominent ridge with blood vessels and extraretinal fibrovascular proliferations (extending from ridge into vitreous)
- Stage 4 3: Partial retinal detachment
- 4A: extrafoveal
- 4B: foveal
- Stage 5: Total retinal detachment
- Plus disease 3 = tendency to progression, poor prognostic sign
- dilated veins and tortuous arteries in at least two quadrants
- no pupil dilation
- massively congested iris vessels
- vitreous opacity
- increasing pre-retinal and vitreous haemorrhages
- “Pre-plus”: is defined by abnormal dilatation and tortuous vessels, not yet sufficient to be called plus disease
- Weekly follow-up necessary until regression or progression to threshold disease
- Threshold disease:
- Blindness in 50% without therapy
- 5 continuous or 8 non-continuous clock hours of extraretinal neovascularisation (stage 3) in zone 1 or 2 associated with plus disease
- Therapy required: laser therapy of avascular immature retina within 48-72h
- Aggressive (posterior) ROP (A-ROP) 3:
- Posterior location in zone I or posterior zone II, plus disease, ill-defined nature of the retinopathy, rapidly progressing
- If untreated, usually leads to stage 5
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Management
- usually both eyes are treated (unless the opposite eye has minimal/no ROP)
- should be done within 48-72h
- Laser therapy in type 1, watch & wait in type 2 (according to ETROP study)
- Type 1 (laser therapy)
- Zone 1, all stages with plus disease
- Zone 1, stage 3 without plus disease
- Zone 2, stage 2+3 with plus disease
- A-ROP
- Type 2 (watch & wait)
- Zone 1, stage 1+2 without plus disease
- Zone 2, stage 3 without plus disease
- Technique: treat the entire avascular area anterior to the demarcation line, avoid the fovea, burns near confluent / max. 0.5 burn-width apart, cloud grey appearance
- Type 1 (laser therapy)
- anti-VEGF therapy (Ranibizumab 0.2mg) as an alternative
- for zone I and posterior zone II
- for zone II/III (except posterior II) laser therapy recommended
- avoid if any sign of pericular infection!
- Technique: under anaesthesia, 30g needle, 0.02ml syringe, 1-1.5mm from limbus, caution: needle not too anteriorly because of large cristalline lens; examine fundus with dilated pupils after injection for adverse effects
- for zone I and posterior zone II
Follow-up (without therapy)
- 6 months (optional)
- 12 months (mandatory)
- every 6 months in the 2nd year of life
- annually from 3 – 6 years of age
- from 6 years on if any ocular problems
Follow-up (after laser therapy)
- Local therapy: e.g. Dexafree UD (Dexamethason) 4x/d + Mydriaticum gtt (Tropicamid) 2x/d for 1 week
- After approx. 1 week: Examine anterior segments for adverse effects, disease regression?
- after 2 weeks: Disease regression?
- if not and laser incomplete: repeat laser treatment
- if not and laser complete: consider rescue treatment with anti-VEGF
- after 3-4 weeks: disease regression?
- after 2-3 months, 6 months: Retinal examination
- 12, 18, 24 months, thereafter annually until at least 5 years: orthoptic evaluation (visual acuity, strabismus, refraction in cycloplegia), examination of retina
Follow-up (after anti-VEGF)
- after 1-2 days and 5-7 days: Examine anterior segments for adverse effects, disease regression?
- then screening for disease reactivation (new Plus, new extraretinal vessels)
- 1x/week for 4 weeks
- 2-weekly for 12 weeks
- 4-weekly for 8-16 weeks, (longer for A-ROP)
- thereafter at 12, 18, 24 months, then annually until at least 5 years: orthoptic evaluation (visual acuity, strabismus, refraction in cycloplegia), examination of retina
- If no regression <1-2 weeks or reactivation during the course: laser therapy recommended (alternatively, repetition of anti-VEGF possible).
Prognosis
- Risk of ROP requiring treatment based on gestational age (weeks) 4: 24 (14.5%), 25 (7.3%), 26 (2.7%), 27 (1.1%), 28 (0.5%), 29-31 (0.06%), total 1.2%.
- Spontaneous regression occurs in approx. 80% of ROP patients
- Significantly increased risk (approx. 2/3 of all treated patients) of ocular problems: Myopia (with laser approx. 1/3 of patients with approx. -5dpt.), strabismus, reduction in visual acuity.
- Average visual acuity (after successful retinal surgery) at stage 4: >0.1 to light perception, at stage 5: light perception to no light perception
Sources
- AWMF Leitlinie Augenärztliche Screening-Untersuchung bei Frühgeborenen
- EyeWiki Retinopathy of Prematurity
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)
- Good WV; Early Treatment for Retinopathy of Prematurity Cooperative Group. Final results of the Early Treatment for Retinopathy of Prematurity (ETROP) randomized trial. Trans Am Ophthalmol Soc. 2004;102:233-250.
- Treating Retinopathy of Prematurity in the UK, Clinical Guidelines 2022, The Royal College of Ophthalmologists
- 1 translated from © Luzerner Kantonsspital, www.kispi-wiki.ch, Authors: Dr. med. M. Fontana, Dr. med. Christoph Amstutz, Dr. med. Maria Helfenstein, Valentina Da Crosta
- 2 © 2020 London School of Hygiene & Tropical Medicine (CC-BY-NC-SA 4.0)
- 3 Molinari A, Weaver D, Jalali S. Classifying retinopathy of prematurity. Community Eye Health. 2017;30(99):55-56. PMID: 29434438; PMCID: PMC5806220. © 2017 Andrea Molinari, Dan Weaver and Subhadra Jalali, Creative Commons Attribution Non-Commercial License
- 4 Gerull R et al. Incidence of retinopathy of prematurity (ROP) and ROP treatment in Switzerland 2006-2015: a population-based analysis. Arch Dis Child Fetal Neonatal Ed. 2018 Jul;103(4):F337-F342. doi: 10.1136/archdischild-2017-313574