Change Language German
Definition
- Angle closure: Blockage of the trabecular meshwork by the peripheral iris with obstruction of aqueous humor outflow.
- Definitions:
- Primary Angle Closure Suspect (PACS): ≥2 quadrants of iridotrabecular contact (ICT), normal intraocular pressure (IOP), no peripheral anterior synechiae (PAS), no evidence of glaucomatous optic neuropathy
- Primary Angle Closure (PAC): Iridotrabecular contact resulting in peripheral anterior synechiae and/or raised IOP, no evidence of glaucomatous optic neuropathy.
- Primary angle-closure glaucoma (PACG): Iridotrabecular contact causing glaucomatous optic neuropathy.
- initial examination +/- elevated IOP, +/- PAS
Aetiology
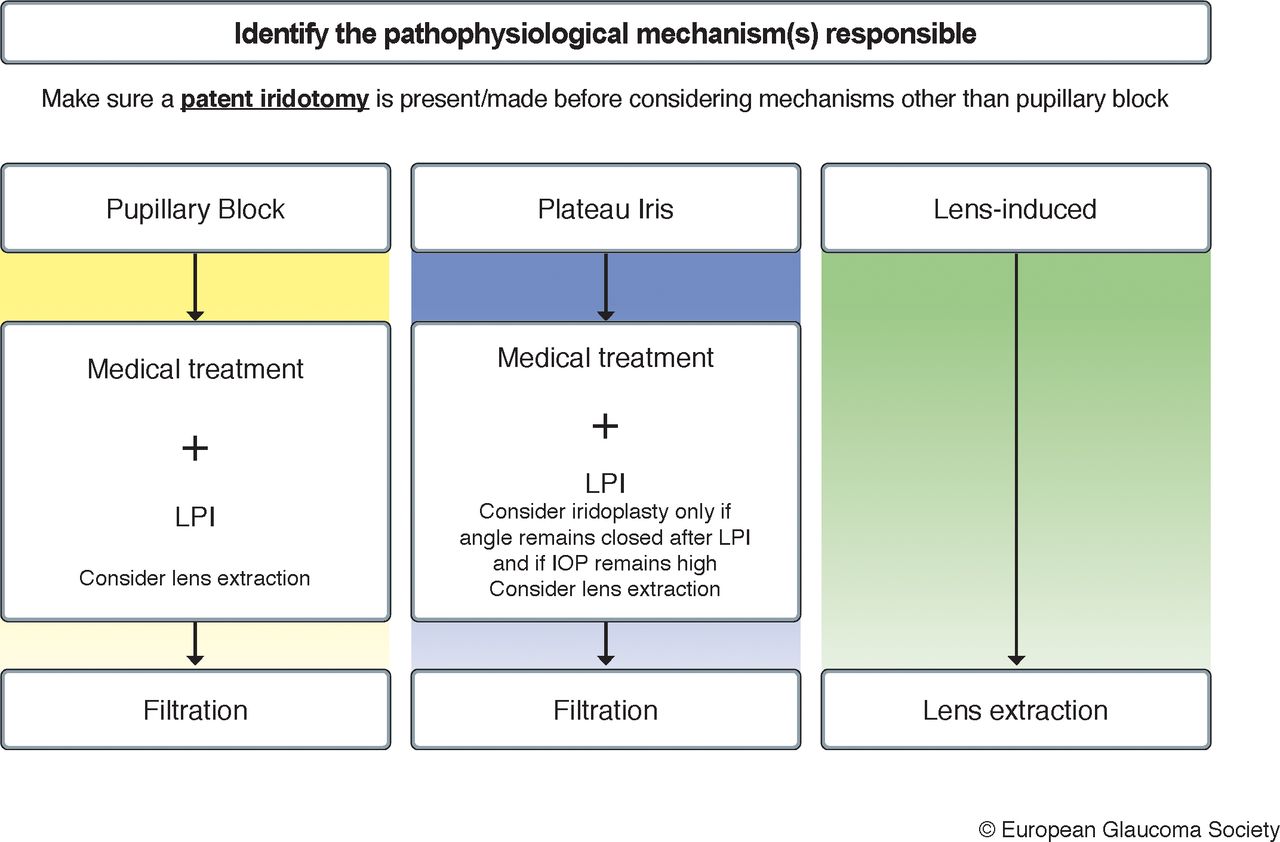
- Primary:
- Pupillary block: Protrusion of the iris and iridotrabecular contact
- Iris-induced angle-closure (without pupillary block): plateau iris configuration
- Differential diagnosis of secondary causes:
- Lens-induced: phacomorphic glaucoma, anterior lens subluxation
- Retrolenticular: malignant glaucoma, tumor
- Inflammatory: due to anterior synechiae in uveitis/inflammation
- Medication-induced: Topiramate, sulfonamide
- Neovascular glaucoma
- Membrane formation: e.g., ICE syndrome, posterior polymorphous corneal dystrophy
- Anomaly: e.g., Axenfeld-Rieger syndrome, Peters anomaly
Symptoms and Findings
- Acute Angle Closure Attack
- Pain: mild to severe eye and/or headache
- Decreased vision (vision often 0.1 – hand motion), halos, foggy vision, eye redness
- Nausea, vomiting
- Possible triggering factors: e.g., watching TV/smartphone in a dark room, drug-induced mydriasis (rarely miosis), acute emotional stress, sometimes systemic medication
- Findings: elevated IOP (50 – 100mmHg), conjunctival injection, corneal oedema, shallow anterior chamber, non-reactive mid-dilated pupil; fellow eye usually also with shallow chamber angle
- Post-acute angle closure attack:
- Lower IOP, Descemet’s folds, choroidal folds
- Later: iris atrophy with spiral configuration, irregular pupil, posterior synechiae, glaucoma flecks
- May have chronic or intermittent course
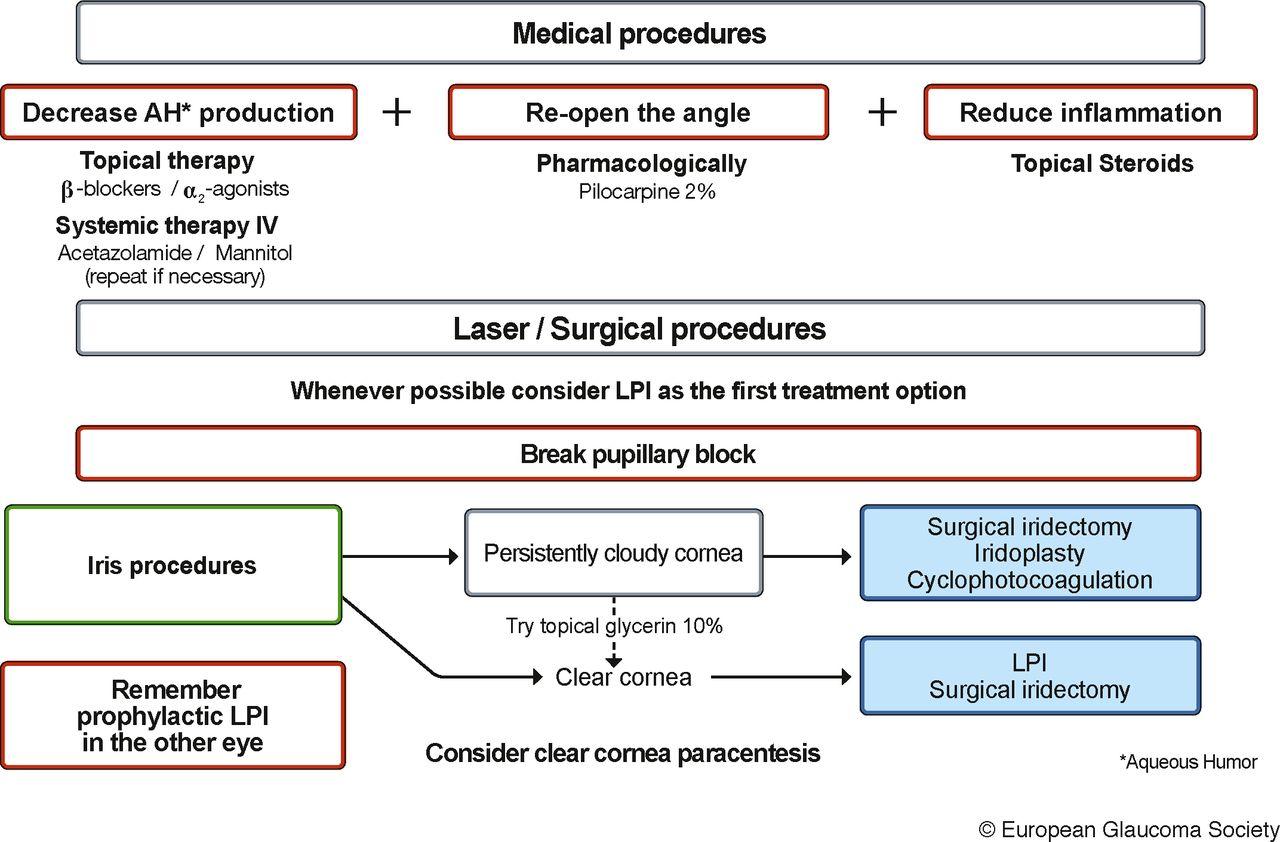
Treatment of Acute Angle Closure Attack
- EGS Guidelines 5th Edition Management of acute primary angle closure attack
- EGS Guidelines 5th Edition Management of chronic angle closure
- The patient should assume a lying position -> the lens shifts backwards
- Medical therapy:
- Timolol eye drops 0.5% 2x/day / Cosopt eye drops 2x/day
- Alphagan eye drops 2x/day
- Spersacarpine 2% eye drops
- Cave: Only if there is no phacomorphic component or malignant glaucoma!
- Diamox i.v. max. 3x500mg/day
- Consider Mannitol i.v. 1x250ml 20% solution as a short infusion over 20-30 minutes
- Cave: Consult with an internist in case of heart/kidney diseases
- Pred forte eye drops 3x within 15 minutes, then 4-6x daily
- Manual measures:
- Indentation of the chamber angle with a contact lens
- Diagnostic: iridotrabecular contact/synechiae?
- Therapeutic: improvement of outflow
- Indentation of the chamber angle with a contact lens
- YAG laser iridotomy
- If the cornea is cloudy, prepare with 10% glycerin eye drops
- Prophylactically also on the fellow eye!
- Alternatively, surgical iridectomy
- Consider paracentesis if there is no reduction in pressure with medication
- Consider cataract surgery for phacomorphic component
{kind=link}
{kind=link}
Treatment after the Attack
- Continue pressure-lowering therapy, e.g., Cosopt eye drops 2x/d or Timoptic 0.5% eye drops 2x/d
- Diamox orally up to 4x 250mg (dose depending on eye pressure)
- Pred Forte eye drops 4x/d for 5-7 days in case of inflammatory reaction
- Spersacarpine 2% every 4 hours, reduce to 3x/d from the 3rd day after the attack
Follow-up
- Within 1-2 days, then weekly checks for 4 weeks
- Subsequently, glaucoma screening (including OCT, visual field)
Sources
- EyeWiki Primary vs. Secondary Angle Closure Glaucoma
- European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition,
- Licensed under a Creative Commons License Attribution-NonCommercial 4.0 International CC BY-NC 4.0 DEED
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Kalla Gervasio MD, Travis Peck MD et al; Lippincott Williams&Wilkins; 8th Edition (2021)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; John E Salmon MD; Elsevier; 9th Edition (2019)