Definition
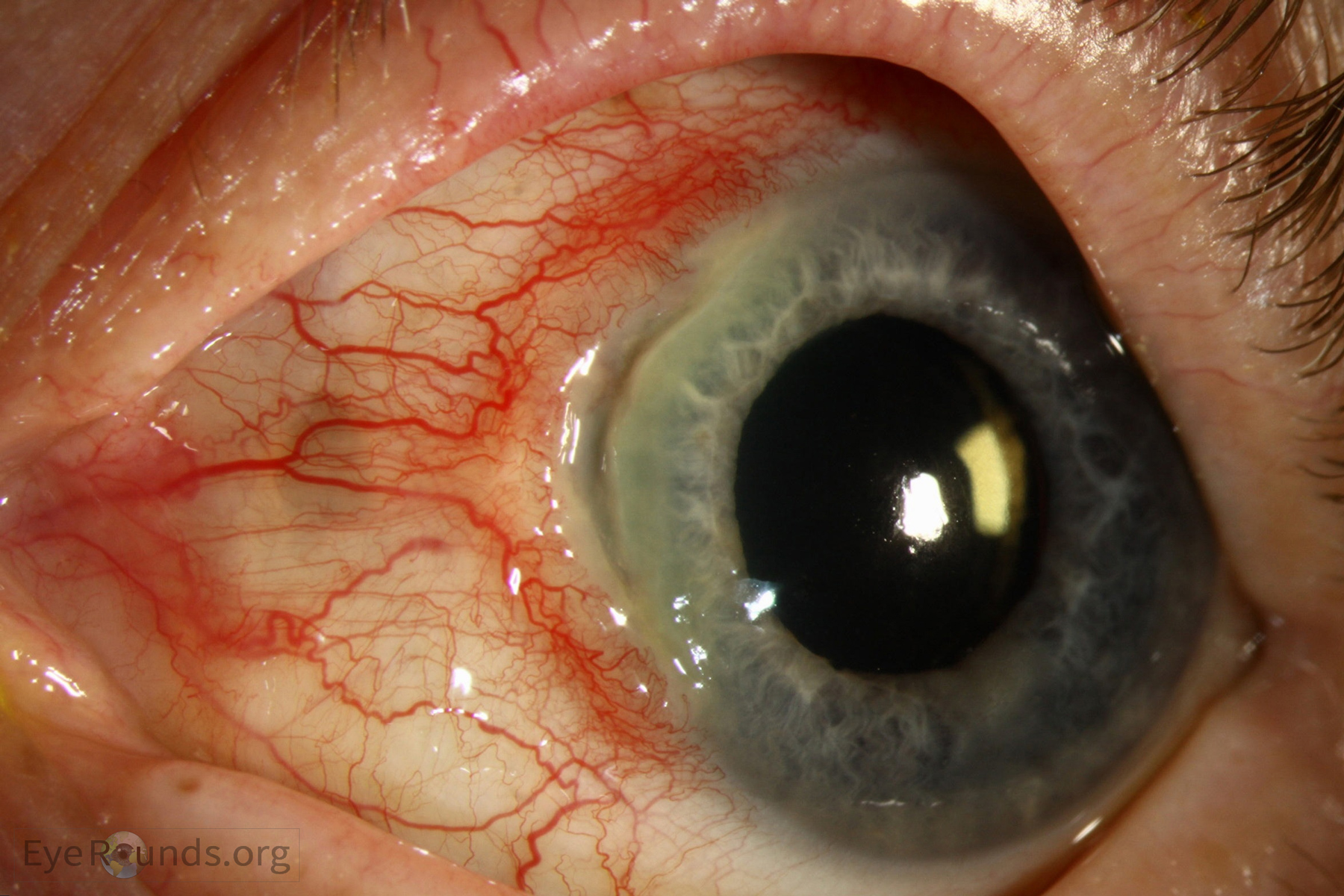
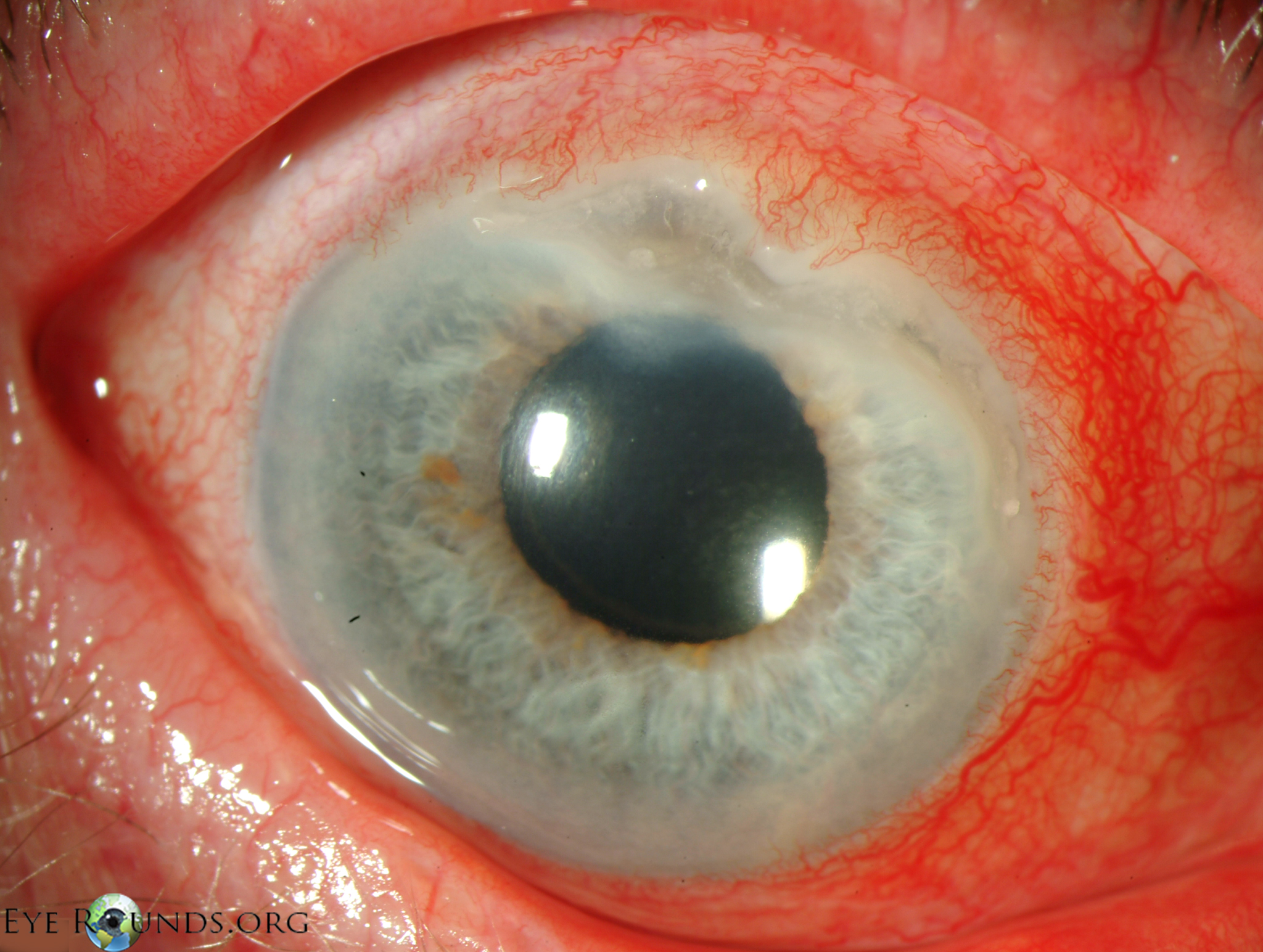
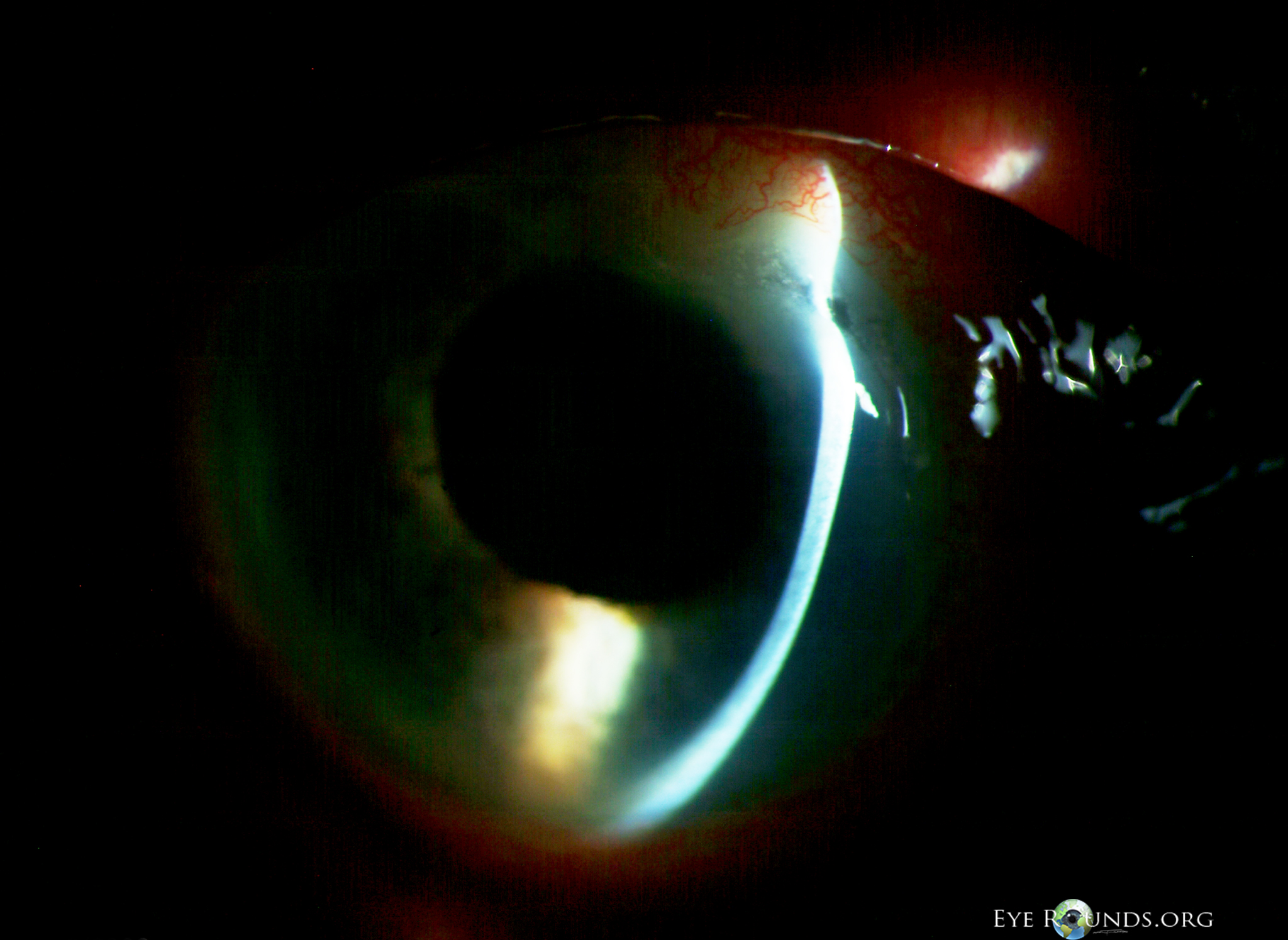
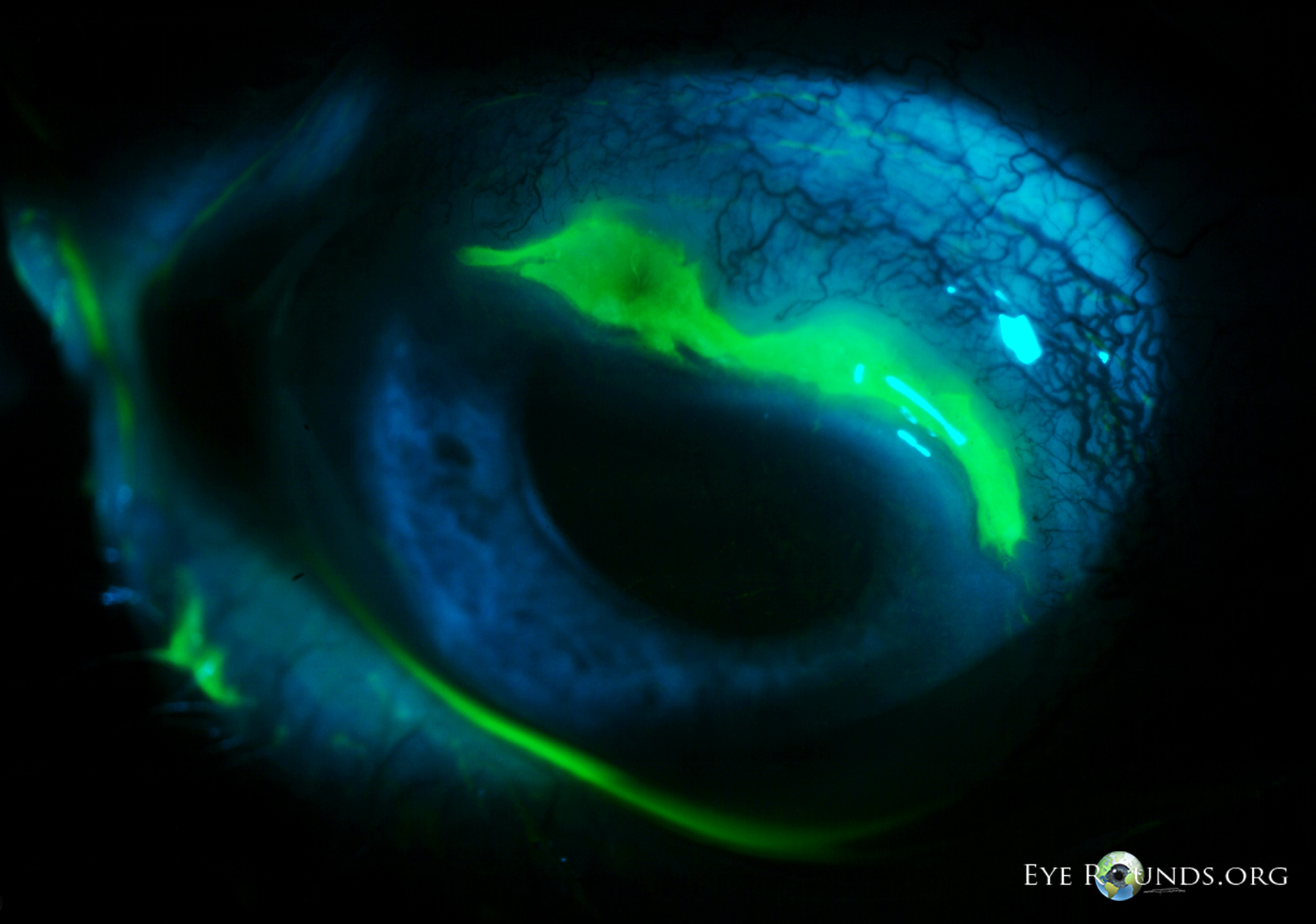
- Peripheral corneal thinning ± sterile infiltrate or ulcer
Differential Diagnoses
- Peripheral Ulcerative Keratitis (PUK)
- Group of inflammatory diseases leading to peripheral corneal thinning
- Unilateral or bilateral
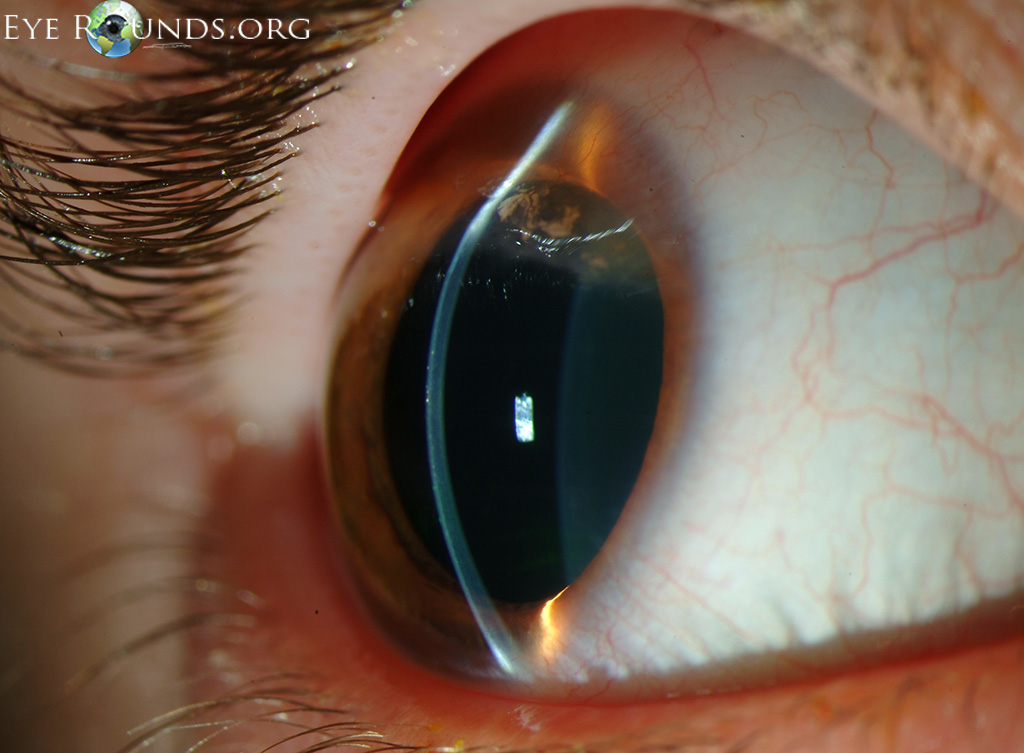
- Crescent-shaped ulceration and stromal infiltration at the limbus, epithelial defect. Circular and occasionally central spread 1 2 3 4
- Mostly limbitis, episcleritis, scleritis. Perforation can occur.
- Often associated with dry eye
- Systemic comorbidities must be investigated!
- Rheumatoid arthritis (most common)
- Granulomatosis with Polyangiitis (second most common)
- Relapsing Polychondritis
- Systemic lupus erythematosus
- Mooren’s Ulcer
- Special form of PUK without scleritis, by definition idiopathic without local or systemic underlying disease, diagnosis by exclusion!
- Unilateral or bilateral
- Severe pain is typical
- Peripheral stromal ulcerations with epithelial defect, central lesion with overhanging edge, usually starting nasally or temporally with circular and later central spread; infiltrations at the periphery, vascularisations.
- Terrien’s Marginal Degeneration
- Corneal Dellen
- Localized, mostly oval corneal thinning; usually next to a raised lesion
- Caused by drying -> lubricating drops
- Pellucid Marginal Degeneration
- Marginal keratitis
- Rule out infectious ulcer -> bacterial keratitis / fungal keratitis
- Ocular Rosacea
- Senile Furrow Degeneration
- decreasing width of the peripheral cornea between the arcus senilis and limbus
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Work-up
- History: especially systemic (rheumatic) or ocular pre-existing conditions?
- Complete slit-lamp examination including fundoscopy (Cotton-Wool spots? Signs of posterior scleritis?)
- consider Schirmer test
- Laboratory tests: Complete blood count, CRP, ESR, RF, anti citrullinated protein antibodies (ACPA), ANA, ANCA
- corneal swab when infectious aetiology is suspected
- consider scleritis – workup
Treatment
- Local (usually not sufficient!)
- Intensive lubrication, punctum plugs, ciclosporin gtt or autologous serum eye drops
- bandage contact lens
- Floxal UD (Ofloxacin) 3-4x/d, topical steroids, e.g., Pred Forte gtt (prednisolone)
- Systemic
- Systemic high-dose corticosteroids/immunosuppression (interdisciplinary with rheumatologist)
- consider oral tetracyclines, e.g., Doxycycline 100mg 2x/d (anti-collagenase activity)
- Surgical
- for small lesions, consider conjunctival resection at the limbus near the lesion
- consider lamellar keratoplasty, amniotic membrane transplantation
Sources
- EyeWiki Peripheral Ulcerative Keratitis
- EyeWiki Mooren´s Ulcer
- EyeWiki Terrien’s Marginal Degeneration
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)
- Yagci A. Update on peripheral ulcerative keratitis. Clin Ophthalmol. 2012;6:747-754. doi:10.2147/OPTH.S24947
- 1,2,3,4,5,6 von Eyerounds.org, © The University of Iowa; Licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License.