Change Language German
Clinical Findings
- Ocular myasthenia gravis:
- Main Signs: Fatigability and variability
- often worsening towards evening
- Ptosis
- Diplopia: Can mimic various forms of ophthalmoplegia
- Facial muscle weakness
- Nystagmus: Noted in extreme gaze positions
- Main Signs: Fatigability and variability
- Generalised myasthenia gravis: Additionally presents with chewing weakness, dysphagia, dysarthria, dyspnoea
- Lee’s 5P:Symptoms not caused by masthenia gravis
- Pain
- Proptosis (exception with associated thyroid eye disease)
- Paraesthesias
- Perception (visual acuity decrease, visual field defects)
- Pupil involvement
Work-up
- Lab tests: Acetylcholine receptor antibodies, anti-MuSK antibodies, +/- anti-Titin antibodies
- Rest test/Ice test
- Tensilon test (Edrophonium)
- Side effects include sweating, nausea, vomiting, hypersalivation, fever, increased IOP
- Antidote: Atropin 0.5mg.
- CT Thorax: To rule out thymoma (70% have thymic hyperplasia, 10% have a thymoma)
- Consider Single-Fiber EMG: Shows fatigue with repetitive stimulation.
- Thyroid Function Tests: 5% of patients develop Graves’ disease!
Differential Diagnoses
- Myotonic dystrophy
- Chronic Progressive External Ophthalmoplegia (CPEO)
- Ptosis of other aetiologies
- Eaton-Lambert Syndrome: Paraneoplastic, associated with small cell lung cancer, impaired pre-synaptic release of ACh, no improvement with Edrophonium
Treatment
- in collaboration with neurology
- Mestinon (Pyridostigmine): An acetylcholinesterase inhibitor
- Titration scheme: e.g., start with 60mg once daily, increasing the dose every 3 days up to 4x60mg
- Caution: If gastrointestinal symptoms (diarrhea, cramps) occur, wait or decrease the dose for a few days before increasing again
- if Mestinon is not sufficient:
- Steroids: e.g., 10mg Spiricort daily for 3 months, then taper off very slowly (high doses can worsen myasthenic symptoms).
- If no response, increase Spiricort to max 20mg/day
- Annual bone density measurement recommended
- Alternative Treatments: Imurek, Cellcept, Rituximab, IVIG (Privigen infusion), Plasmapheresis, Thymectomy (in case of thymoma, consider in generalised form)
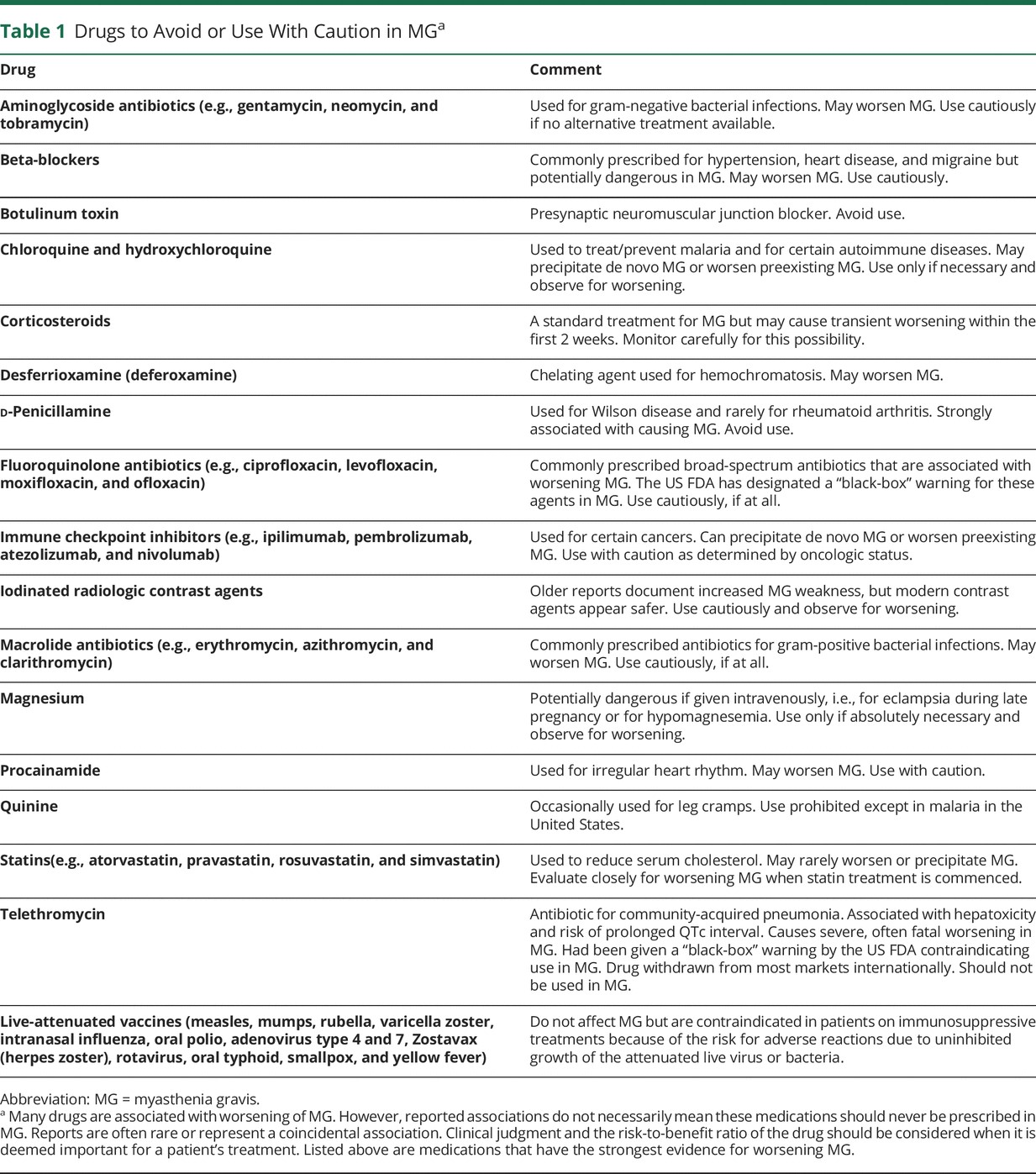
Medications to avoid
- List , 1
- not exhaustive, includes medications with the highest evidence of risk
- Antibiotics
- Aminoglycosides (e.g., Gentamicin, Neomycin, Tobramycin)
- Fluoroquinolones (e.g., Ciprofloxacin, Levofloxacin, Moxifloxacin, Ofloxacin)
- Macrolides (e.g., Erythromycin, Azithromycin, Clarithromycin)
- Telithromycin
- Beta-blockers
- Botulinum toxin
- Chloroquine and Hydroxychloroquine
- High-dose corticosteroids
- D-Penicillamine
- Desferrioxamine
- Immune checkpoint inhibitors (e.g., Ipilimumab, Pembrolizumab, Atezolizumab, Nivolumab)
- Iodine-containing contrast media
- Intravenous magnesium
- Procainamide
- Statins (e.g., Atorvastatin, Pravastatin, Rosuvastatin, Simvastatin)
{kind=link}
Follow-up
- First check approximately 1 week after treatment initiation (to assess medication tolerance)
- Patient education: In case of systemic manifestations of myasthenia gravis (chewing weakness, dysphagia, dysarthria, dyspnoea), seek immediate medical attention
Video by Dr. Andrew G. Lee
Sources
- EyeWiki Myasthenia Gravis
- Ocular Myasthenia Gravis by Dr. Andrew G. Lee
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)
- 1 International Consensus Guidance for Management of Myasthenia Gravis; 2020 Update;