Change Language German
Findings
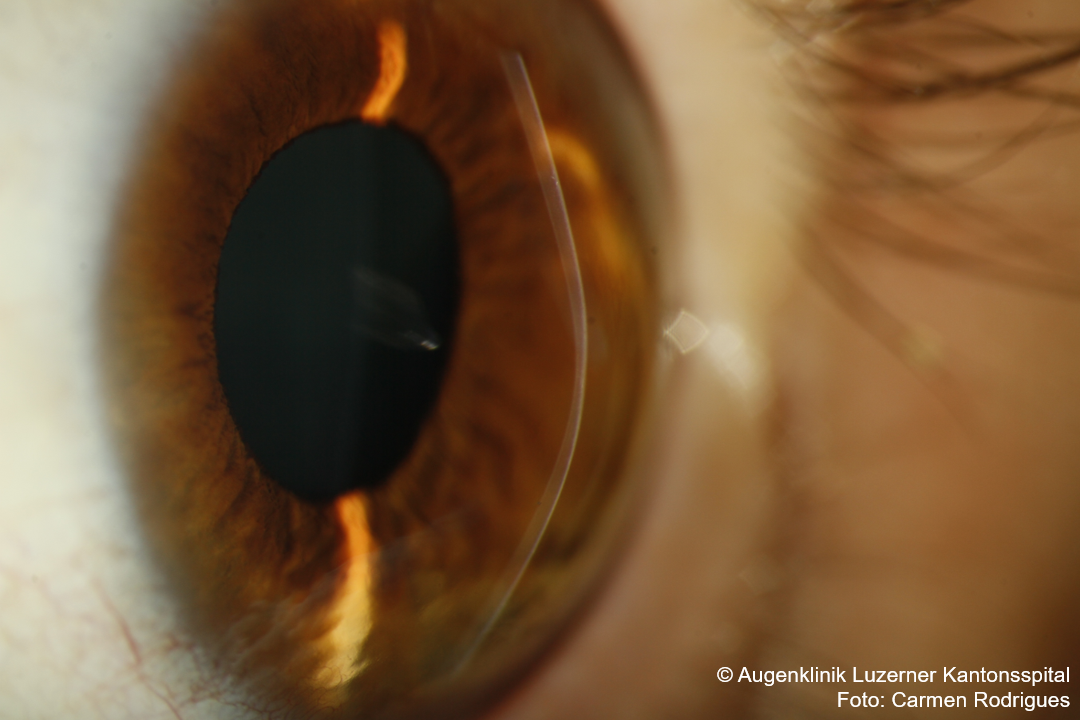
- progressive stromal thinning and protrusion
- Irregular astigmatism; scissor reflex on retinoscopy
- Vogt’s striae = very fine, vertical deep stromal striations, disappear with pressure applied over the eyeball
- Oil drop sign in direct ophthalmoscopy
- Fleischer ring = iron deposits around the base of the keratoconus
- Central corneal opacity = tears in Bowman’s membrane and scarring (indicating progression of the keratoconus)
- Salzmann’s nodule-like superficial scarring = Caused by rubbing from rigid contact lens
- Munson’s sign = protrusion of the lower eyelid on downgaze
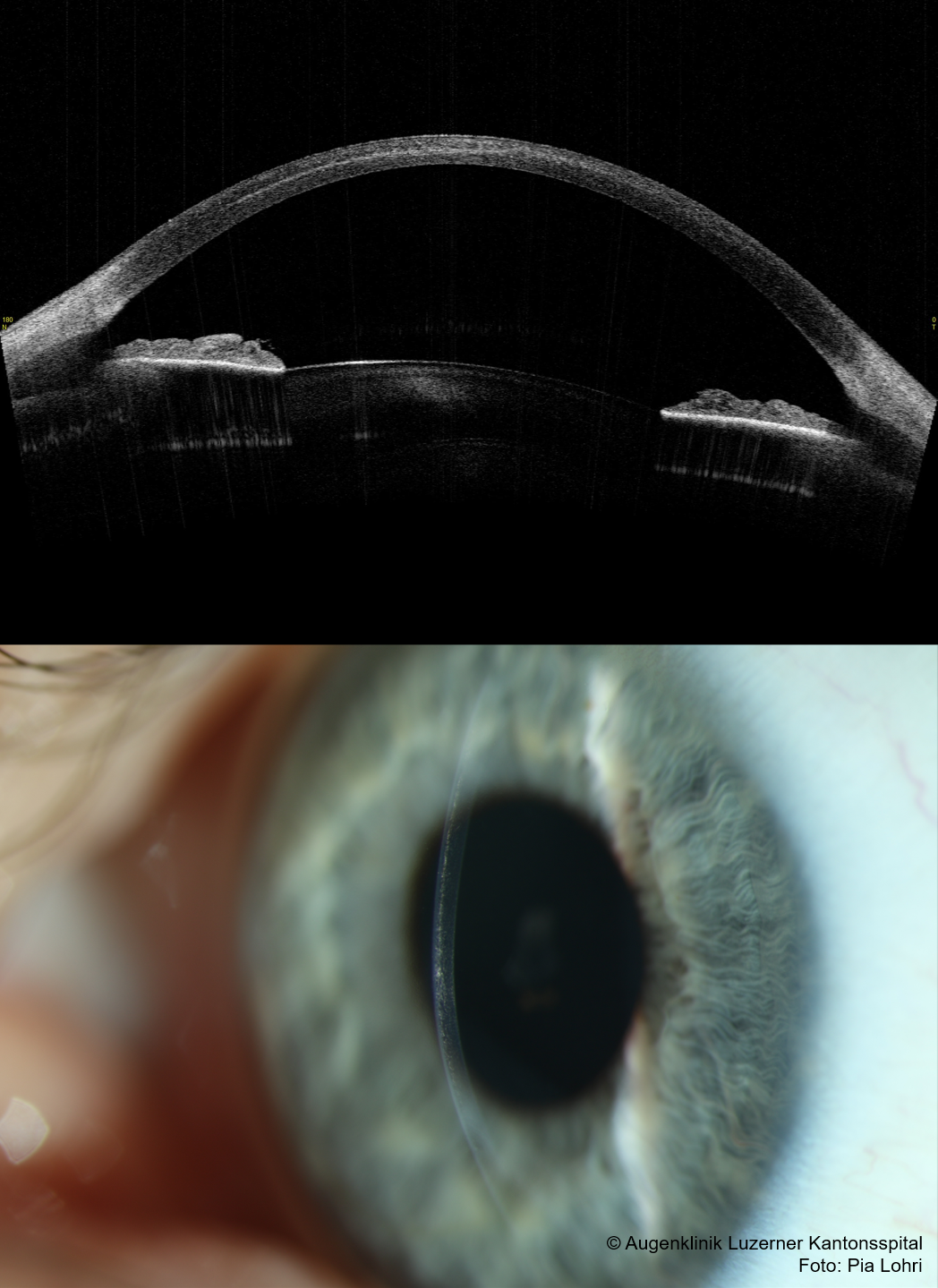
- Hydrops = Descemet’s tear -> corneal oedema (usually closes on its own within 6 – 12 months)
{kind=link}
{kind=link}
Work-up
- Clinical findings
- Topography:
- Shape: island-shaped elevation of the posterior surface > anterior surface = central ectasia
- Corneal thickness/thinnest point
- K-value: increase in refractive power (Kmax > 48dpt. not physiological)
- D-value (Belin-Ambrosio coefficient): summarising overall parameter -> severity of keratoconus (the higher the value, the more pronounced the keratoconus)
- Subclinical keratoconus
- typically abnormal posterior elevation, abnormal pachymetry
- Visual acuity normal, as anterior corneal surface typically not yet affected!
Management
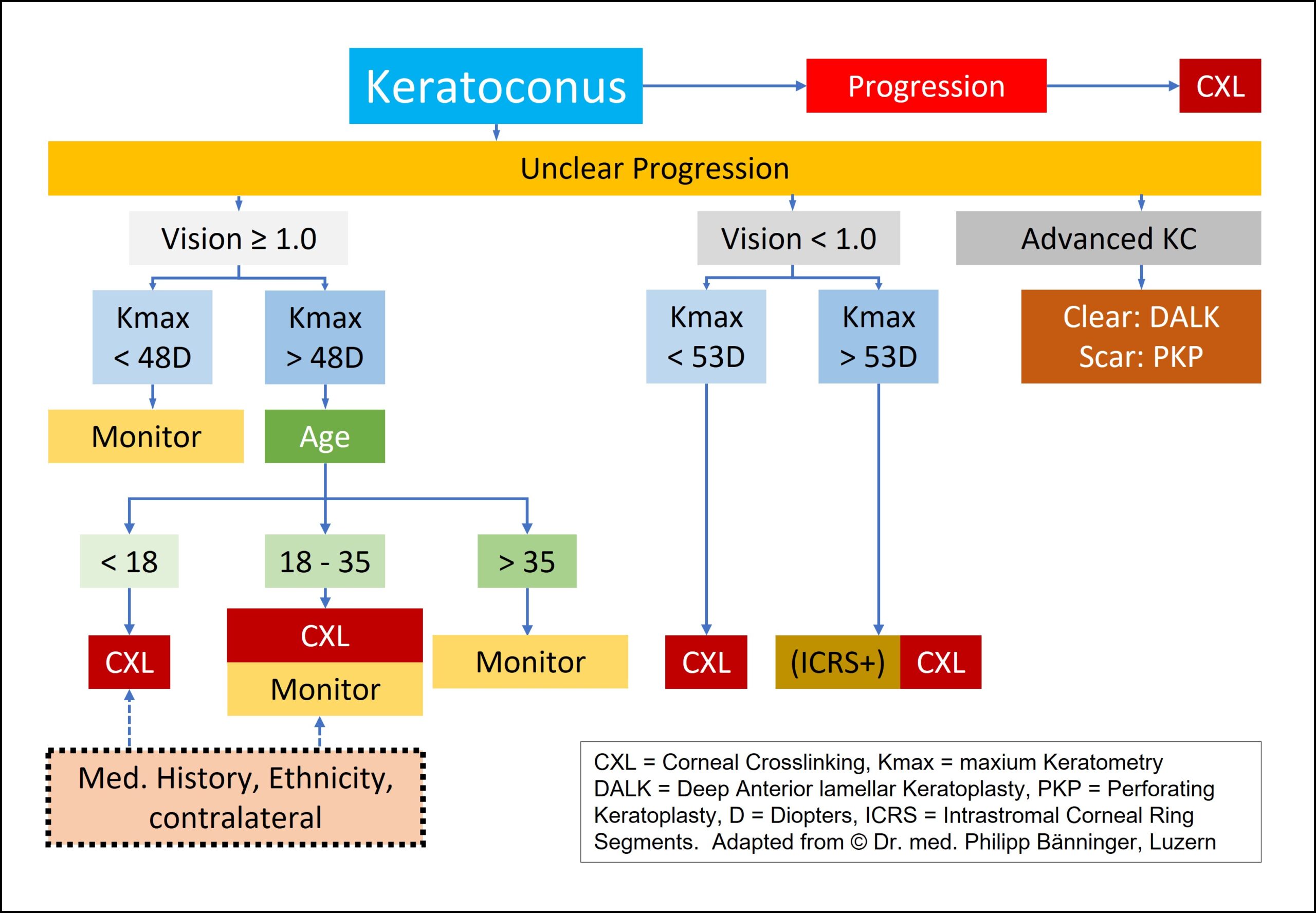
- Flowchart
- Instruct patients to avoid eye rubbing!
- Rigid contact lenses or mini scleral lenses -> possible up to Kmax of ∼70
- Corneal Crosslinking (CXL) with riboflavin eye drops
- Indication: Progression of keratoconus ectasia
- Objective: Stabilisation/prevention of progression
- Methods: epi-on = epithelium is not abraded beforehand or epi-off = with preceding epithelial abrasion
- Keratoplasty: DALK or PKP (fitting of a mini-scleral lens after PKP after 4-6 months at the earliest).
- (implantation of an intracorneal ring segment (Intacs))
- in acute hydrops:
- Consider NaCl Dispersa eye drops 5% 3-5 times daily (although usually not sufficient)
- Consider cycloplegia (pain management)
- Consider bandage contact lens
- Consider bandage or glasses to protect against trauma/eye rubbing
- usually spontaneous healing within 6-10 weeks
- Consider corneal suture, air/gas injection
- PKP not indicated in acute phase!
{kind=link}
{kind=link}
Follow-up
- in young patients (between the ages of 12 and 18) and questionable progression of keratoconus: follow-up after 3 months, if stable 6-monthly
- in older patients (> 20 years): follow-up every 6-12 months
- Relevant progression of keratoconus is rare in patients above 35/40 years
- Reliable progression parameters:
- Form
- K-value (Kmax not very reliable)
- D (Belin-Ambrosio coefficient)
- Corneal thickness
- Astigmatism (not so meaningful, as average)
Possible concomitant diseases
- Down’s, Turner’s, Ehlers-Danlos and Marfan syndromes, atopy, osteogenesis imperfecta, mitral valve prolapse
- Pregnancy
- Hyper-/hypothyroidism
Pellucid marginal degeneration
- Important differential diagnosis!
- might be a different phenotype of the same disease
- painless peripheral corneal thinning inferiorly
- crescent 1-2mm wide band inferiorly (typically from 4-8 o’clock), approx. 1mm distance from limbus
- intact epithelium
- no inflammation visible
- corneal protrusion above the thinnest part
- no Fleischer ring, no Vogt striae, hydrops very rare
- Corneal topography: crab claw-like pattern with high astigmatism and “steepening” of inferior cornea
- Therapy identical to keratoconus; PKP however more difficult due to peripheral thinning
Sources
- Flowchart (adapted): Dr. med. Philipp Bänninger, Management Keratokonus, 18th Lucerne Eye Meeting – 20. Juni 2015
- EyeWiki Keratoconus
- EyeWiki Ectasia Risk in Topography
- National Keratoconus Foundation
- EyeWiki Pellucid Marginal Degeneration
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)