Change Language German
Clinical Presentation
- Pseudotumor cerebri
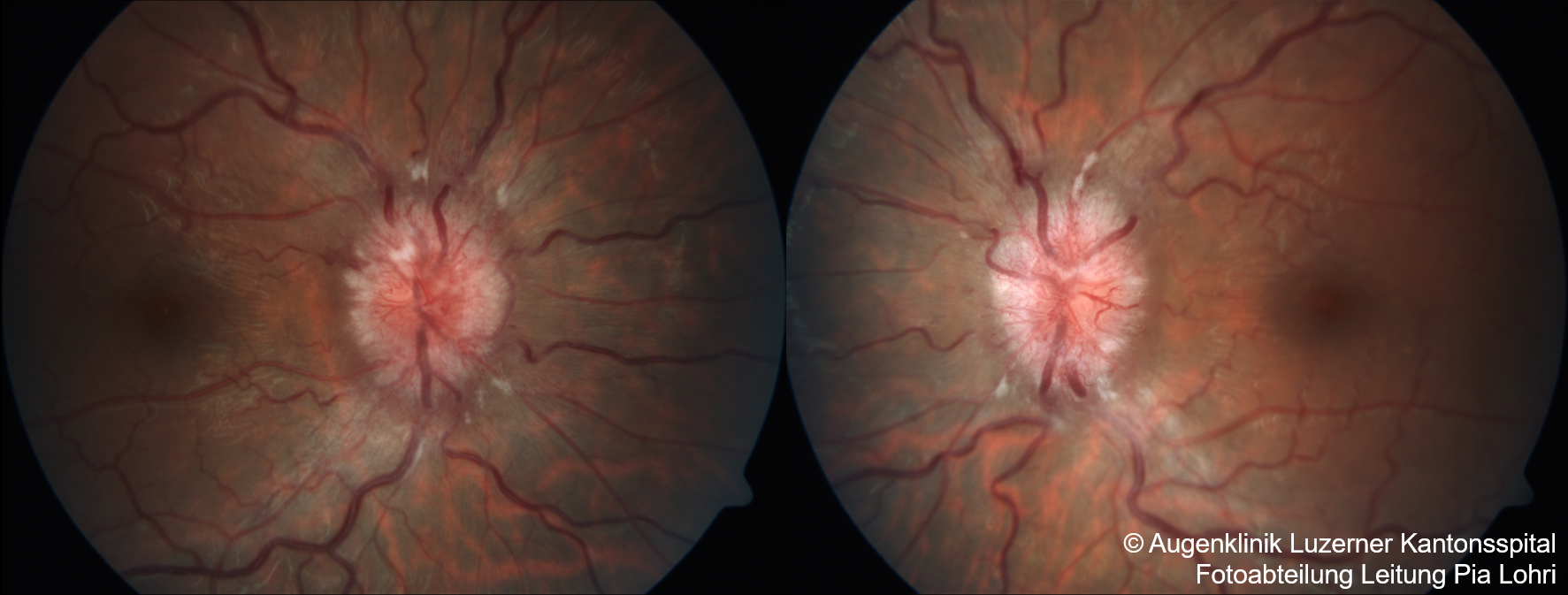
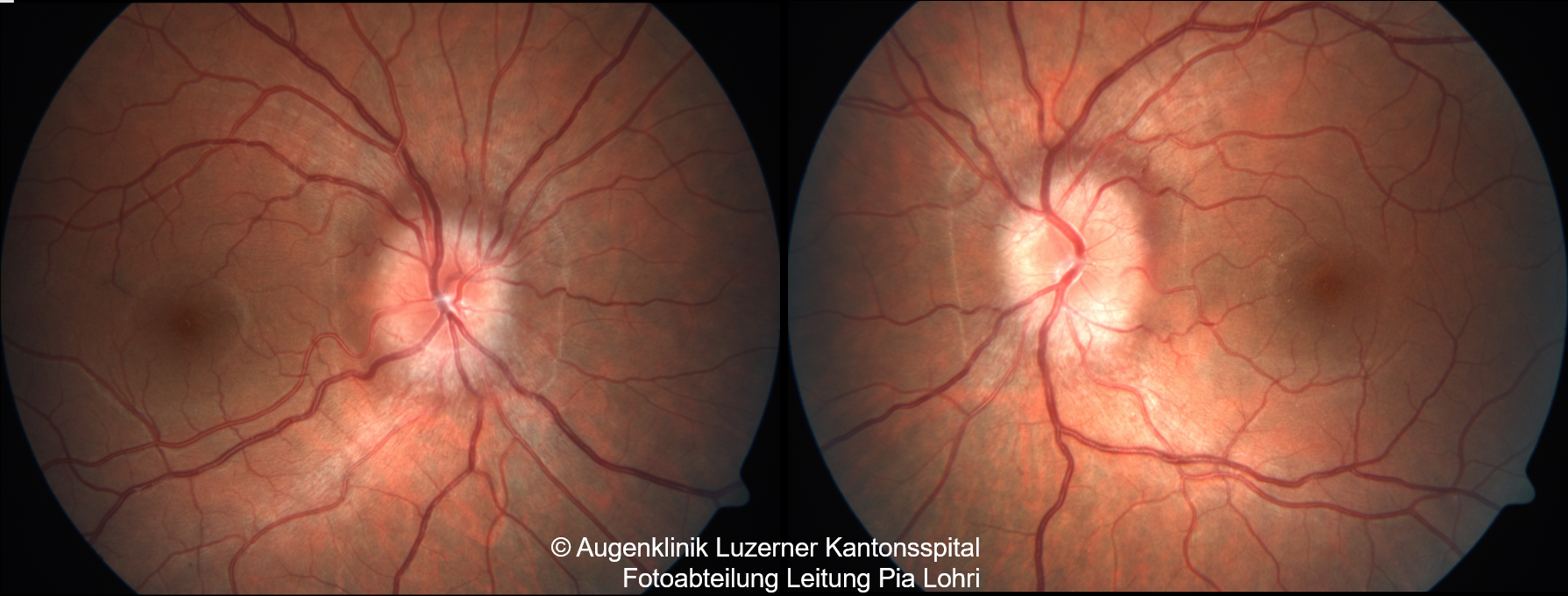
- Bilateral papilledema (acute stage: optic nerve head swelling 1 2, chronic: optic atrophy )
- Loss of spontaneous venous pulse (absent in 20% of normal population)
- Transient visual obscurations
- +/- diplopia (due to sixth nerve palsy)
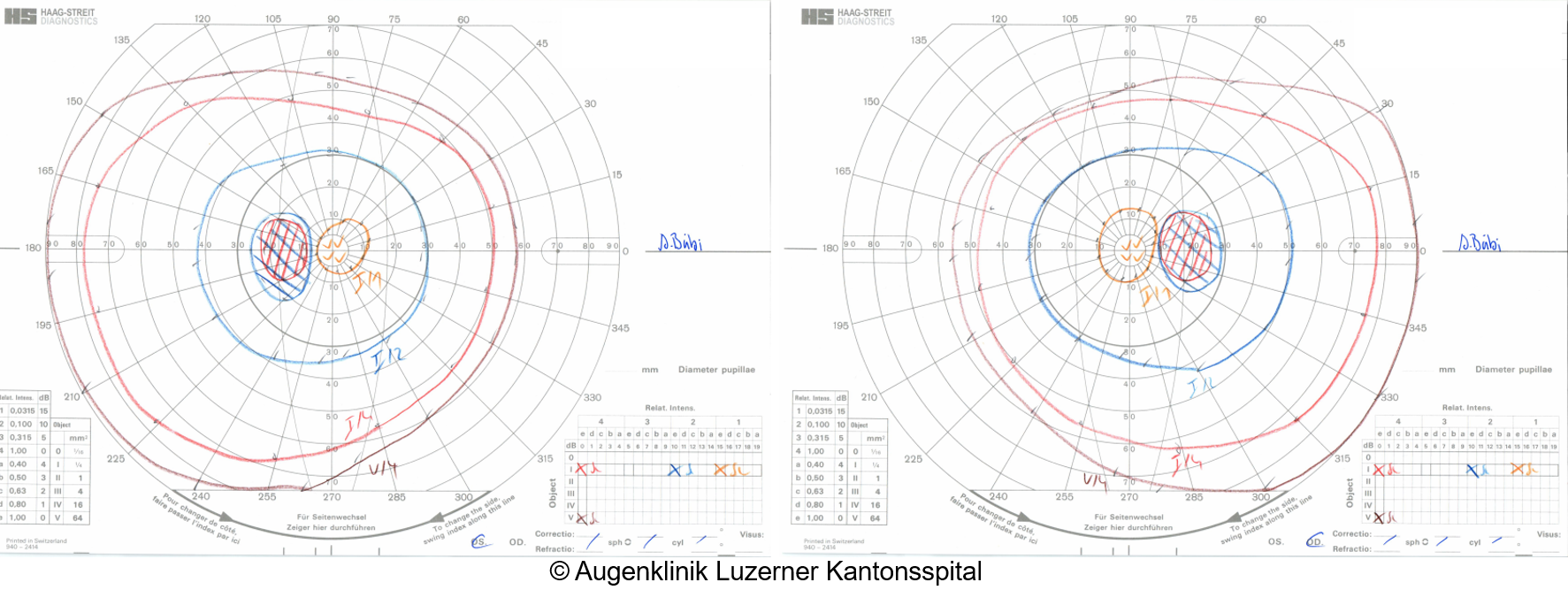
- Enlarged blind spot in visual field examination or arcuate scotomas; other defects possible, concentric visual field restriction suggests optic nerve damage
- Headaches, typically occipital and positional (worsens when lying down)
- Nausea, vomiting
- Pulsatile tinnitus
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Work-up
- Emergency CT angiography of the head to rule out a venous sinus thrombosis
- MRI angiography with venography within 1 week if no acute symptoms
- Blood pressure (malignant hypertension?)
- Laboratory tests: TSH, fT3, fT4, electrolytes, creatinine, vitamin A, B12, albumin, ASAT, ALAT, iron status (to rule out secondary causes of pseudotumor cerebri) + INR (for lumbar puncture)
- Further history:
- Medication intake: steroids, oral contraceptives, vitamin A, tetracyclines, nalidixic acid, lithium, isotretinoin
- Personal history: COPD, pregnancy, neck surgery, weight gain?
- In women: regular menstruation? (indications of PCOS?)
- Follow-up (within 1-2 weeks):
{kind=link}
Management
- Diamox (acetazolamide) therapy for about 1 year, consider tapering off earlier if only mild papilledema and successful rapid weight loss
- Start with 2x 250mg/day in the first week, then 4x 250mg/day (+ potassium effervescent tablets 30mmol/day)
- First follow-up after 1 month -> Diamox can be increased to max. 2g daily if insufficient response (initial monthly potassium checks, then every 3 months)
- Tapering off: relatively quickly over a few weeks, after stopping Diamox therapy, follow-ups initially every 6-12 weeks
- Topiramate therapy (alternative, if Diamox is not tolerated or if mainly headaches are present -> also a migraine medication)
- Start with 25mg in the evening, increase by 25mg/day each week to 2x50mg/day (up to a maximum of 200-250mg daily). Potassium supplementation needed from 100mg/day, similar to Diamox therapy.
- Gradually increase Topiramate to 2x 50mg:
- Start with 25mg in the evening, then increase by 25mg/day each week
- Dose can be increased up to 200-250mg daily
- From 100mg daily, potassium supplementation is necessary, similar to Diamox therapy
- Mandatory reliable contraception and adequate fluid intake, especially during exercise
- Regular laboratory or medication checks are not mandatory
- Alternatively, Furosemide (Lasix), initial kidney function check recommended
- Weight loss: target 10-15% reduction, nutritional counselling
- If advanced visual field defects or pregnancy (Diamox and Topiramate contraindicated)
- Evaluate optic nerve sheath fenestration or lumbo-peritoneal shunt placement
- If sinus stenoses and non-response to medication:
- Refer patient to neuroradiology for transstenotic pressure gradient measurement and assessment of the need for sinus stenting
Sources
- EyeWiki Pseudotumor cerebri (idiopathic intracranial hypertension)
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)
- 1, 2 Eyerounds.org, © The University of Iowa; Licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License (CC BY-NC-ND 3.0).