Change Language German
Findings
Epithelial keratitis
- Punctate epithelial keratitis
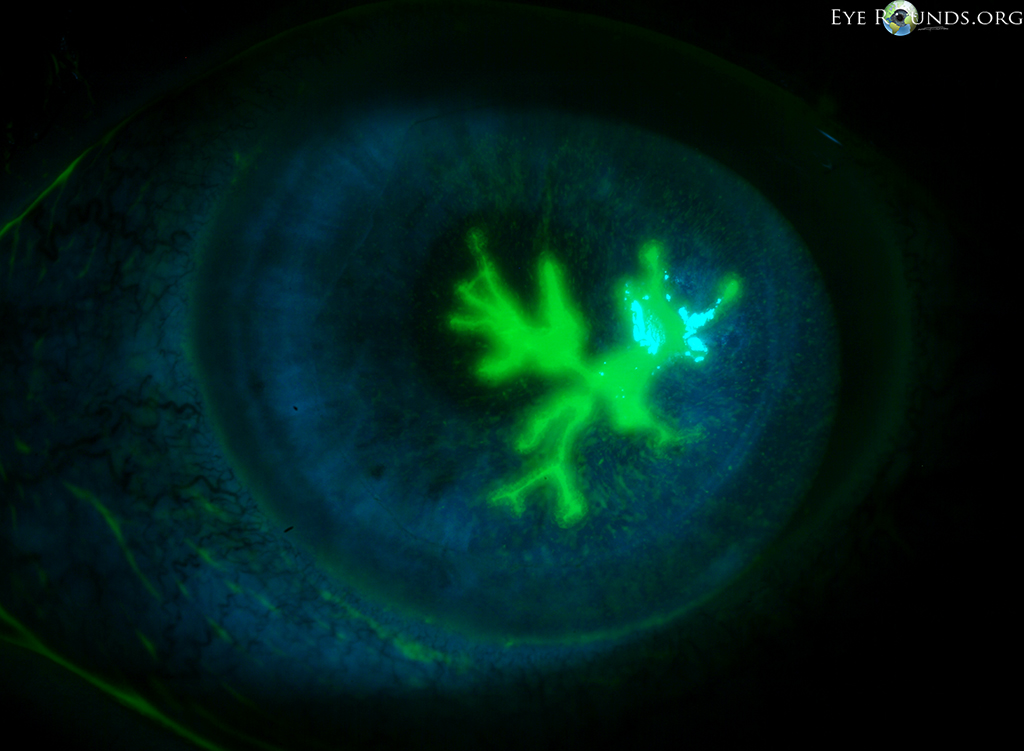
- Dendrites: fluorescein-positive branching epithelial ulcer, blunt ends with “terminal bulbs” 1 2
- Geographica: larger epithelial defect with dendritic margins 3
- Corneal sensation typically reduced
{kind=link}
{kind=link}
{kind=link}
Neurotrophic ulcer
- see Neurotrophic Keratopathy
- Persistent epithelial defects
- May lead to stromal melting and perforation
Stromal keratitis and endotheliitis
- Immune reaction to viral antigens
- Stromal opacities
- Disciform (round) stromal/epithelial oedema above localised endotheliitis
- typically with endothelial precipitates
Keratouveitis
- See Anterior Uveitis
- Definition
- Keratouveitis = Anterior uveitis + keratitis
- Uveitis anterior = without keratitis
- Fine granulomatous endothelial precipitates, anterior chamber cells/flare, patchy iris atrophy, increased IOP (due to iridocyclitis)
Acute retinal necrosis (ARN)
- see separate article
Work-up
- Medical history: previous episodes
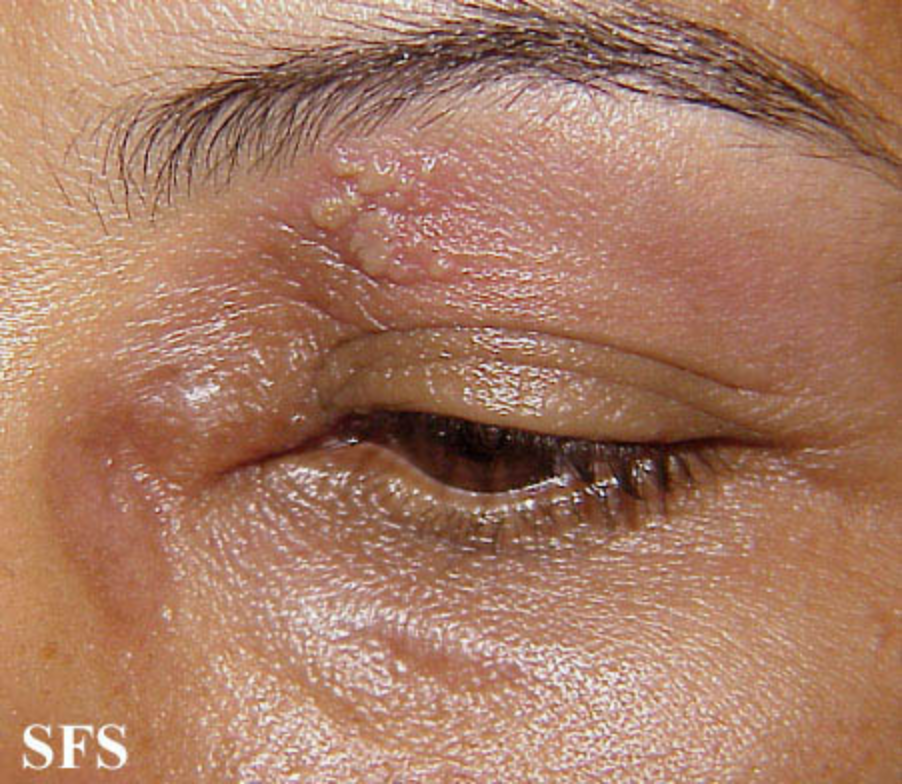
- Skin findings: vesicles in V1 suggest VZV 4, if only around the eye: HSV more likely 5
- Slit lamp examination
- Cornea: Epithelium: Dendrites? Ulcer? Stromal infiltrates? Stromal thinning? Corneal vascularisations? Precipitates? Corneal Sensation?
- Anterior chamber: Cells? Flare?
- Iris: Transilluminations? (HSV: diffuse; VZV: patchy) Posterior synechiae?
- IOP: asymmetric? Elevated? Low?
- CAVE: check corneal sensation first
{kind=link}
{kind=link}
Diagnosis
- A smear is not mandatory if the clinical signs are typical (e.g. epithelial dendrites)
- Corneal PCR swab or abrasion (e.g. with a Kimura spatula) in the area of the dendrites to remove loose epithelium, thereby reducing viral load.
- If necessary, anterior chamber puncture for PCR: in recurrent episodes with uveitis in which HSV has never been detected.
Therapy
Epithelial keratitis
- Virgan Gel (Gangciclovir) 5x/d
- alternatively Zovirax ointment (Aciclovir) 5x/d
- alternatively, Valtrex p.o. (Valaciclovir) 3x500mg daily (in case of surface problems or if application of ointments is difficult)
- In case of large epithelial defects, consider prophylactic antibiotic treatment (e.g. Floxal SDU (Ofloxacin) 3x/d)
- In case of keratouveitis (see Uveitis Anterior)
- Consider Scopolamine gtt 2x/d to prevent posterior synechiae
- Cauteously consider steroid drops (e.g. Pred forte gtt (Prednisolon) / Dexafree SDU (Dexamethason) depending on anterior chamber cells (CAVE: officially contraindicated in epithelial ulcers)
- in case of non-healing epithelial defects
- bacterial superinfection?
- Acanthamoebae?
- Poor compliance?
- Epithelial toxicity of the drops? -> Switch to Valtrex p.o. (Valaciclovir) and intensive lubrification with drops without preservatives (e.g. Benzalkonium chloride).
Stromal keratitis and endotheliitis
- Combination of local steroids and prophylactic Valtrex p.o. (Valaciclovir)
- e.g. Pred forte gtt (Prednisolon) 4xtgl.
- In case of epithelial defect, combined preparation with antibiotic, e.g. Tobradex gtt (Tobramycin + Dexamethason) 4x/d
- Valtrex 3x500mg for 1-2 weeks, then reduce and treat prophylactically for several months (e.g. Valtrex (Valaciclovir) 2x250mg).
- Reduce cautiously, depending on the frequency of recurrences, long-term therapy should be considered
- CAVE: Check creatinine for long-term therapy
- Reduce cautiously, depending on the frequency of recurrences, long-term therapy should be considered
Neurotrophic ulcer
Acute retinal necrosis (ARN)
- see separate article
Follow-up
- Within 1 week: Response to therapy?
- Thereafter 1-2-weekly:
- Assessment of: Epithelial defect? Depth of the ulcer? Vascularisation? Anterior chamber cells? IOP?
- Reduce steroid drops slowly (over months to >1 year).
- Long-term therapy with Valtrex (Valaciclovir) often necessary, evaluation of the minimum required dose (note down at which dose a relapse occurs!)
Sources
- EyeWiki Herpes simplex Epithelial Keratitis
- EyeWiki Herpes simplex Stromal Keratitis, Endotheliitis
- EyeWiki Herpes simplex Interstitial Keratitis
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7. Auflage (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8. Auflage (2015)
- 1, 2, 3 von Eyerounds.org, © The University of Iowa; Licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License (CC BY-NC-ND 3.0).
- 4, 5 https://www.atlasdermatologico.com.br/