Change Language German
Technique
- Direct gonioscopy:
- in a supine position, usually in the operating theatre
- Indirect gonioscopy:
- Can be performed at the slit lamp
- Lenses:
- Goldmann (1- or 3-mirror contact glass): use a gel (e.g. Lacrinorm), no indentation possible
- Posner, Sussman, Zeiss: Indentation possible, no gel needed, may use lubrifying drops / topical anesthetic drops
- Perform in a darkened room
- Topical anaesthesia (e.g. Oxybuprocaine or Tetracaine gtt.)
- Ask the patient to look straight ahead (may look upwards to insert the lens)
- Use the smallest possible light slit, not too bright.
- Assessment of the anterior chamber angle: usually easiest inferiorly, start there; then assess all four quadrants (rotate 360° with Goldmann lens)
- consider indentation in case of a closed anterior chamber angle
- To distinguish appositional closure and detect peripheral anterior synechiae (anterior chamber angle remains closed)
- with Posner, Sussman or Zeiss lens; apply slight pressure to cornea
- Always examine both eyes
Anterior chamber angle anatomy
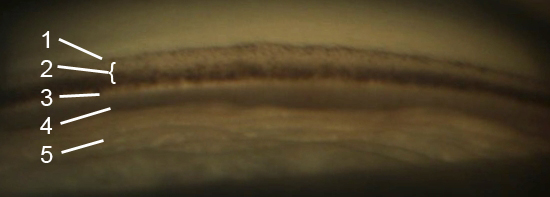
- 1 Schwalbe line = junction of the cornea and trabecular meshwork, to identify use a corneal light wedge: intersection of the reflection of the external corneal surface and the internal surface
- 2 Trabecular meshwork: upper “non-functional” part and lower more pigmented “functional” part
- Schlemm-Kanal: slightly darker line
- 3 Scleral spur: prominent white line / ridge
- 4 Ciliary body band: brown or gray band, can only be seen in deep angles
- Iris processes: small pigmented strands of the iris surface that insert at the level of the scleral spur (found in 1/3 of normal eyes) ≠ peripheral anterior synechiae (wider)
Classification
- Spaeth (most detailled)
- Insertion level of the iris root:
- A: anterior to Schwalbe’s line
- B: posterior to Schwalbe’s line
- C: on the scleral spur
- D: behind the scleral spur
- E: on the ciliary body band
- Angular width of angle recess: 0-40°
- Configuration of the peripheral iris: regular (r), steep (s, anteriorly convex), queer (q, anteriorly concave)
- Pigmentation of the trabecular meshwork: 0 (not pigmented) – 4 (very pigmented)
- Insertion level of the iris root:
- Shaffer
- 0: closed
- 1: very narrow, ≤10°
- 2: narrow, 10-20°
- 3: open, 20-35°
- 4: wide open, 35-45°
- Scheie
- 0: wide open, all structures visible
- I: iris root visible
- II: ciliary body obscured
- III: posterior trabecular meshword not visible
- IV: only Schwalbe’s line visible
- Pigmentation of the trabecular meshwork: 0 (not pigmented) – 4 (very pigmented)
- Peripheral anterior chamber depth (Slit lamp) – Van Herick method
- how deep is the very peripheral anterior chamber, corneal thickness as unit measure, preferably on the temporal side
- 0: iridocorneal contact, angle closure
- 1: <1/4 corneal thickness, angle closure probable
- 2: 1/4 corneal thickness, angle closure possible
- 3: 1/2 corneal thickness, angle closure unlikely
- 4: one corneal thicknesseine or more, angle closure very unlikely
Indications
- Assessment of the anterior chamber angle in glaucoma patients (mandatory at initial diagnosis)
- Open/closed angle in case of elevated IOP
- Neovascularisation of the chamber angle
- Angle recession , iris disinsertion or ciliary body cleft in case of trauma
- Foreign body or lens particle in the chamber angle
- Anomalies of the chamber angle
- Tumour expansion
{kind=link}
{kind=link}
Sources
- EyeWiki Gonioscopy
- Gonioscopy.org – Atlas of Gonioscopy – Excellent Page with lots of examples
- 1 Wikipedia, User: Snoop. Licensed under a CC BY-SA 3.0 DE Deed | Attribution-ShareAlike 3.0 Germany | Creative Commons
- 2, 3, 4, 5 Wikipedia, User: Mick lucas, Licensed under a CC BY-SA 3.0 Deed | Attribution-ShareAlike 3.0 Unported | Creative Commons
- Spaeth Grading System from EGS Guideline 2015
- Youtube Video-Lecture from Dr. Richard. A. Lehrer, MediTred® 2014
- Youtube Video Series (9 parts) from Dr. Adel Abdelshafik
- Youtube Test yourself Gonioscopy from Dr. Adel Abdelshafik, 8 videos with examples