Change Language German
Approach
- Monocular or binocular?
- Monocular: Double vision when 1 eye ist covered: almost always ocular, use pinhole
- Binocular: Double vision disappears when either eye is covered
- If binocular: Constant or temporary double vision?
- If constant double vision: Paretic or restrictive?
- Restrictive: Endocrine orbitopathy? If unclear, consider CT/MRI of the orbit
- Paretic: Slow saccades
- If paretic:
- Supranuclear: Normal doll’s eye maneuver
- Dorsal midbrain syndrome? Progressive supranuclear gaze palsy (PSP)?
- Nuclear: Oculomotor nerve palsy? Trochlear nerve palsy? Abducens nerve palsy?
- Cave: Myasthenia gravis?
- Supranuclear: Normal doll’s eye maneuver
- Eye misalignments (Cover-/Uncover tests)?
Monocular Double Vision
- Eye diseases
- dry eye
- High astigmatism
- Iridotomy/iridodialysis
- Cataract
- Decentered intraocular lens
- Incorrect glasses correction
- Corneal diseases, e.g., keratoconus
- Macular edema
Binocular Double Vision
- Muscle and orbital diseases
- Restrictive myopathies
- Endocrine orbitopathy
- Myositis (restrictive or paretic)
- Mitochondrial myopathy, e.g. chronic progressive external ophthalmoplegia (CPEO).
- Paretic myopathies
- Myositis
- Myotoxicity after retrobulbar or peribulbar anesthesia
- Orbital diseases
- Orbital cellulitis (bacterial, fungal, viral)
- Vascular-related orbitopathies: carotid-cavernous fistula, giant cell arteritis, cavernous sinus thrombosis, orbital ischemic syndrome
- Autoimmune-related inflammations, e.g., granulomatosis with polyangiitis, sarcoidosis, orbital pseudotumor
- Trauma
- Orbital tumors, including lymphoma
- Restrictive myopathies
- Neuromuscular junction disease
- Myasthenia gravis, others: idiopathic, drug-induced (e.g. penicillamine, aminoglycosides, betablockers, chlorpromazine etc.)
- Nerve Diseases
- N. III palsy
- Compressive: Aneurysm (in 1/3 of patients, often at the junction between the internal carotid artery and the posterior communicating artery), tumours (e.g., pituitary tumour, sphenoid wing meningioma), increased intracranial pressure with uncal herniation (non-reactive wide pupils in unconscious patients)
- Ischemic: Atherosclerosis, diabetes mellitus, hypertension, giant cell arteritis
- Inflammatory: Multiple sclerosis, viral, postviral
- Trauma
- N. IV palsy
- Congenital (unilateral, frequent)
- Traumatic (bilateral or unilateral)
- Ischemic (unilateral!): Atherosclerosis, diabetes mellitus, hypertension, giant cell arteritis
- Compressive: Tumours in the midbrain, pineal region, or cavernous sinus
- Inflammatory (rare): Infectious or post-infectious neuritis
- N. VI palsy
- Ischemic (common, unilateral): Atherosclerosis, diabetes mellitus, giant cell arteritis
- Compressive (common, unilateral or bilateral): Sphenoid wing meningioma, internal carotid artery aneurysm in the cavernous sinus, pituitary tumors, nasopharyngeal carcinomas, metastases with invasion of the cavernous sinus
- Inflammatory (rare, unilateral): Sarcoidosis, viral, meningitis, mastoiditis, sphenoid sinusitis
- Increased intracranial pressure of any etiology
- Trauma (unilateral or bilateral)
- Unilateral Multiple Nerve Palsies
- Cavernous sinus syndrome: caused by pituitary apoplexy, cavernous sinus thrombosis, carotid-cavernous fistula, aneurysm of the internal carotid artery, infection, inflammation, tumour
- Orbital apex syndrome: same causes and symptoms as cavernous sinus syndrome but additionally optic neuropathy
- Bilateral Multiple Nerve Palsies
- Bilateral cavernous sinus syndrome
- Bilateral apex syndrome
- Meningitis
- Guillain-Barré syndrome/Miller Fisher syndrome (presumed post-infectious autoimmune demyelinating polyneuropathy, mainly affecting cranial nerves and peripheral motor nerves)
- Wernicke encephalopathy (Thiamine = Vitamin B1 deficiency, leading to degeneration of the oculomotor cranial nerves and vestibular nuclei in the brainstem -> ataxia, confusion, ophthalmoplegia)
- N. III palsy
- Brain Disease
- Supranuclear eye movement disorders (result in gaze palsies characterized by the absence of diplopia and a normal vestibuloocular reflex)
- Horizontal gaze palsy due to lesions in the pons
- PPRF lesion (= pontine paramedian reticular formation: connection to the ipsilateral abducens nerve. Lesion of the PPRF: ipsilateral horizontal gaze palsy).
- MLF lesion = Internuclear ophthalmoplegia (MLF = medial longitudinal fasciculus) -> reduced ipsilateral adduction when looking towards the opposite side and abducens nystagmus of the contralateral eye; adduction is better/normal with convergence!); possible skew deviation, vertical diplopia, direction- and upbeat-nystagmus. Exclude Myasthenia gravis!
- Posterior lesion (pons): preserved convergence
- Anterior lesion (midbrain): WEBINO = wall-eyed bilateral INO: impaired convergence
- Brainstem (midbrain and pons) infarction, tumour, inflammation, infection, or Multiple Sclerosis
- Wernicke encephalopathy
- Pernicious anemia (Vitamin B12 deficiency)
- Ipsilateral combined PPRF and MLF lesion (or ipsilateral abducens and MLF lesion) = one-and-a-half syndrome = Fischer syndrome (only abduction of the contralateral eye is possible, which also has an ataxic nystagmus; vertical eye movements intact).
- Infarction (most common cause)
- Multiple Sclerosis
- Basilar artery occlusion
- Pontine metastases
- Vertical gaze palsy due to midbrain lesions (lesions of the rostral interstitial nucleus of the MLF, which is immediately dorsal to the red nucleus in the midbrain).
- Progressive supranuclear palsy (PSP = progressive supranuclear palsy) = Steele-Richardson-Olszewski syndrome -> a severe degenerative disease = generalized brainstem degeneration with destruction of supranuclear connections to the oculomotor nerve nuclei. Findings: supranuclear gaze palsy, initially primarily affecting downward gaze (and the appearance of vertical saccades) -> “dirty tie” syndrome because patients soil themselves while eating due to not seeing their food (DDs for saccade disorders inferiorly: PSP, Whipple’s disease, Niemann-Pick); with the progression of the disease, upward gaze is also affected; horizontal movements are eventually impaired, and a general gaze palsy develops; extrapyramidal rigor, gait ataxia, and dementia; convergence paralysis.
- Dorsal Parinaud midbrain syndrome (= pretectal syndrome)-> Parallel position in primary position, supranuclear paresis of upward gaze, disturbed convergence, large pupils with light-near dissociation, lid retraction (Collier’s sign), convergence-retraction nystagmus with attempted upward gaze, skew deviation.
- Etiology in 90%: Pineal tumor; others: MS, infarction, trauma.
- Skew deviation (vertical bilateral divergence, concomitant or incomitant, without cyclodeviation, due to an imbalance of prenuclear inputs, i.e., a brainstem lesion, whose cause is not nuclear or fascicular N. III or N.IV palsy).
- Brainstem (midbrain, pons, or medulla) infarction, tumour, infection, inflammation, or MS.
- Horizontal gaze palsy due to lesions in the pons
- Supranuclear eye movement disorders (result in gaze palsies characterized by the absence of diplopia and a normal vestibuloocular reflex)
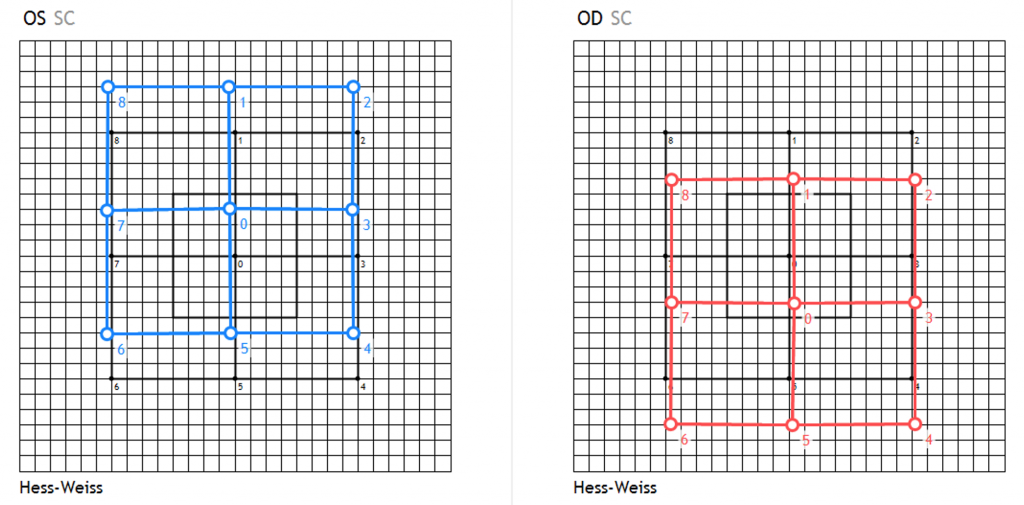
Hess-Weiss of a Patient with Skew Deviation due to Posterior Thalamic Infarction
CAVE:
- In supranuclear brain disorders (PSP, Parinaud syndrome), eye motility during the vestibuloocular reflex (VOR) is less restricted than during intentional eye movements
- In ophthalmoplegias of other etiologies (e.g., CPEO = chronic progressive external ophthalmoplegia), the VOR is equally limited as intentional eye movements
Other Causes of Double Vision
- Decompensated strabismus
- Decompensated phorias
- Convergence insufficiency (primary or secondary; double vision only up close)
- Convergence spasm (primary or secondary; double vision worse in the distance than up close, miosis, increased accommodation)
- Divergence insufficiency (double vision only in the distance)
- Unilateral or bilateral abducens nerve palsy due to a tumour
- Myasthenia gravis (bilateral medial rectus palsy)
- Cerebral diplopia or polyopia: each eye sees the same two (or more) images, and it makes no difference whether the right, left eye is covered or binocular viewing occurs; the double vision persists even when looking through a pinhole. Cause: parieto-occipital tumours, infarction, or migraine.
Sources
- EyeWiki Basic Approach to Diplopia
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7. Auflage (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8. Auflage (2015)
- Clinical Pathways in Neuro-Ophthalmology An Evidence-Based Approach: Stacy Smith; Andrew G. Lee; Paul W. Brazis; Thieme; 3. Auflage (2018)
- The Neuro-Ophthalmology Survival Guide: Anthony Pane; Neil R Miller; Michael Burdon; Elsevier; 2. Auflage (2017)