Change Language German
Overview
Penetrating Keratoplasty (PKP)
- Indication: Any stromal or endothelial corneal pathology, especially bullous keratopathy (pseudophakic, aphakic), keratoconus, scars, Peter’s Anomaly
- Advantages: No interface-associated visual problems
- Disadvantages: Astigmatism, neuropathic keratopathy (delayed wound healing, persistent epithelial defects)
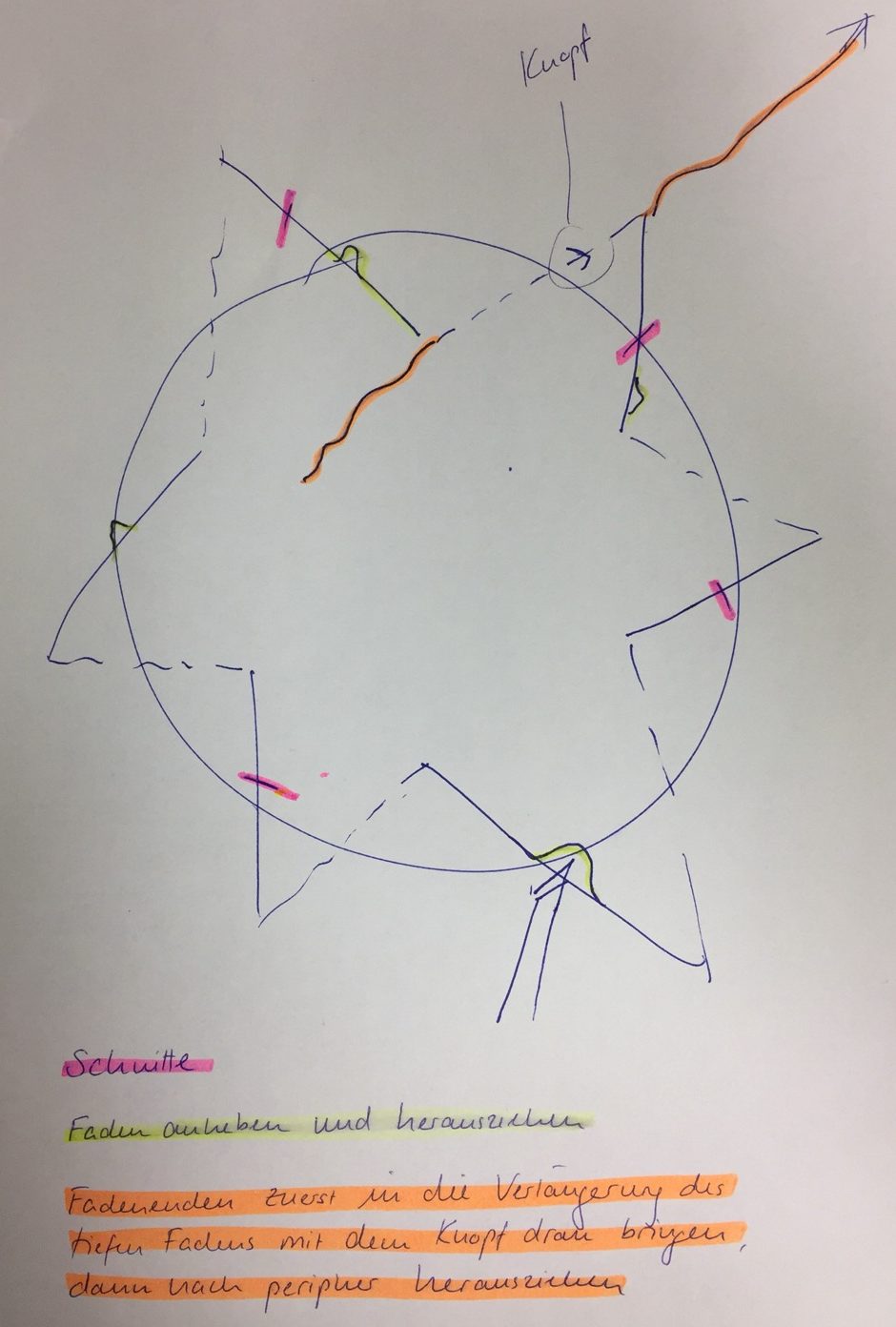
- Suture removal begins after 9-12 months (interrupted sutures) or 12-24 months (continuous suture); removal of a radial suture after PKP (if knot in host cornea) ; after suture removal, e.g., Floxal UD 4x daily for 4-5 days.
{kind=link}
Superficial Anterior Lamellar Keratoplasty (SALK)
- Indication: Superficial stromal dystrophies and degenerations, Salzmann nodules, scars (post-infection/trauma)
- Advantages: Faster visual rehabilitation, reduced risk of rejection
- Disadvantages: Uneven surface, interface vascularisation
Deep Anterior Lamellar Keratoplasty (DALK)
- Indication: Keratoconus, scars after infections, stromal dystrophies not affecting endothelium
- Advantages: Sutures can be removed faster than in PKP due to more stable wound, fewer steroids needed
- Disadvantages: Surface irregularities
Descement Stripping Automated Endothelial Keratoplasty (DSAEK)
- Indication: Endothelial dystrophies, pseudophakic bullous keratopathy, ICE syndrome, failed corneal grafts
- Advantages: Rapid visual rehabilitation, no suture-associated issues, stable corneal surface (less astigmatism), fewer follow-up checks needed, rare need for re-bubbling
- Disadvantages: Stromal haze, subepithelial fibrosis, or irregularity
- Additional: Visual improvement expected within 6 months to 1 year. Patients typically achieve an average visual acuity of 0.63. Average graft survival 6-7 years
Descement’s Membrane Endothelial Keratoplasty (DMEK)
- Indication: Same as DSAEK
- Advantages: Rapid visual rehabilitation (generally better visual outcome than DSAEK), no suture-associated issues, stable corneal surface, reduced risk of immune reaction
- Disadvantages: Stromal haze, subepithelial fibrosis or irregularity, more extensive postoperative follow-ups, more frequent re-bubbling (about 20%)
- Additional: Average graft survival 6-7 year
Transplantatabstossung
- Any corneal layer can be rejected
- Endothelial rejection most common and serious, as loss of endothelial cells leads to decompensation
- Findings (post-PKP):
- Early stage: ciliary vessel injection and anterior uveitis
- Epithelial rejection: Raised epithelial line of abnormal epithelium, usually quiet eye; occurs on average after 3 months; treatment not always necessary
- Subepithelial rejection: Subepithelial infiltrates (= Krachmer spots) in donor cornea
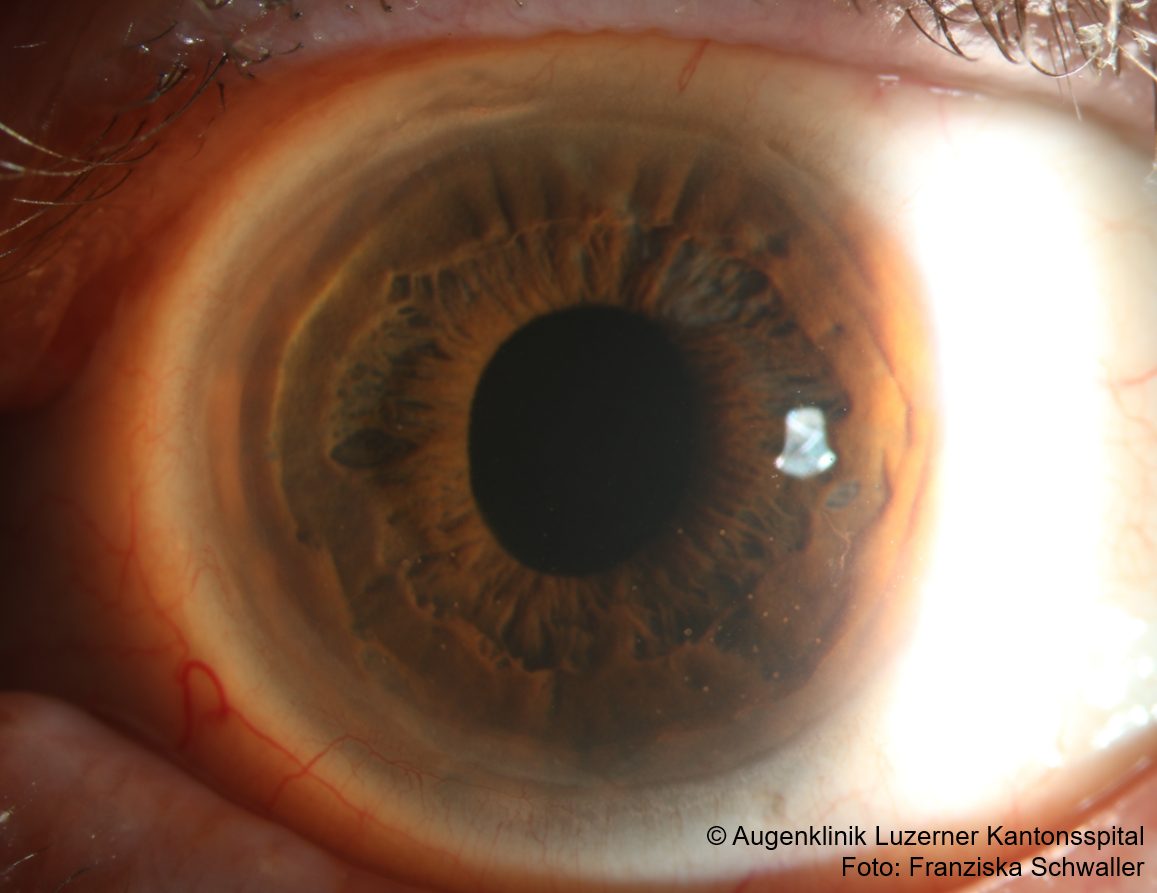
- Stromal rejection: Haze (deep corneal clouding)
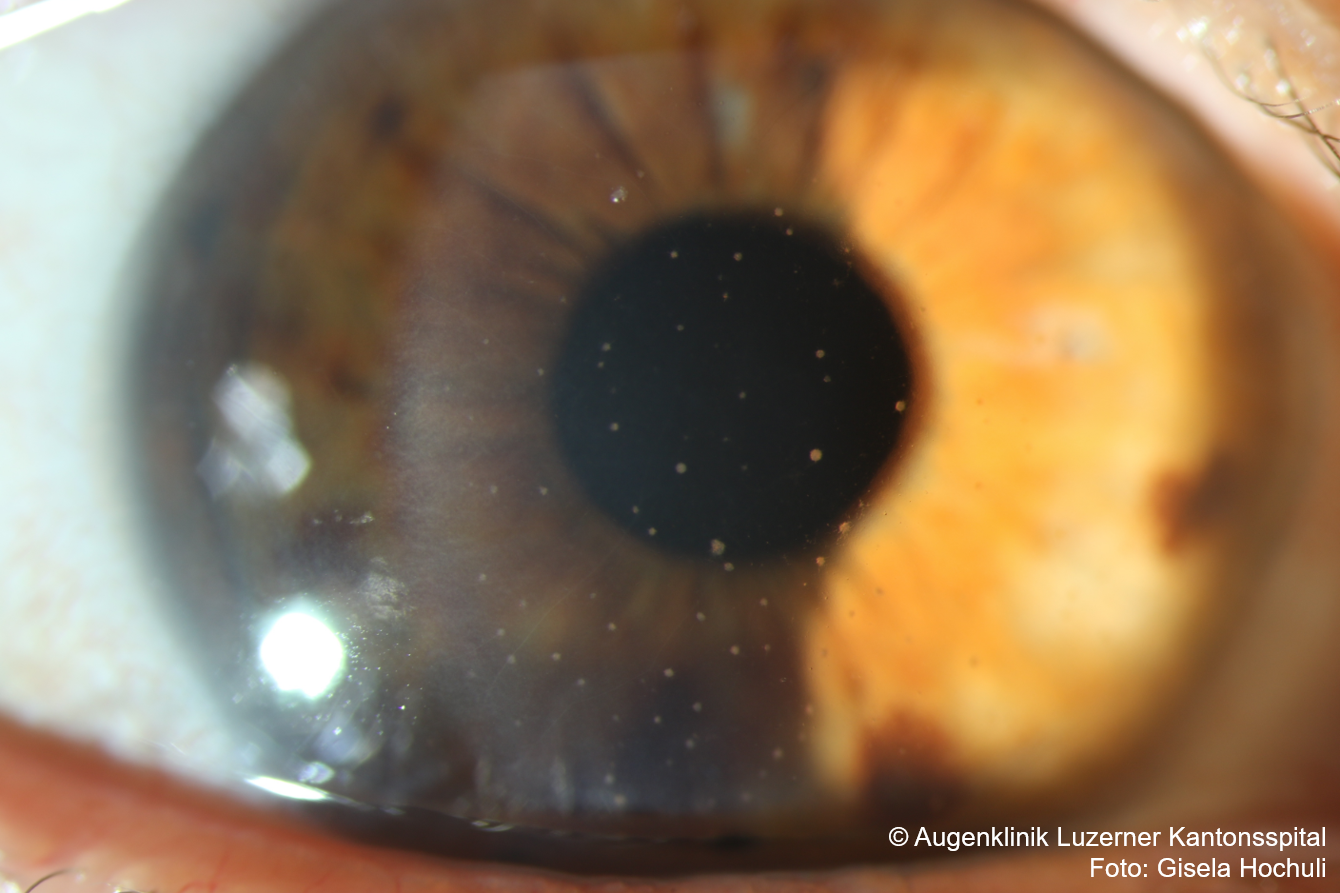
- Endothelial rejection: Endothelial precipitates , typically linear arrangement (= Khadadoust line) associated with inflammation at the transplant edge
- Treatment
- Local steroids: e.g., Pred forte hourly for 24 hours, then Pred forte during the day and Ultracortenol ointment at night for about 2 weeks; then tapering off steroids every 2 weeks to a lifelong minimum dose higher than at the time of rejection
- +/- systemic steroids (1mg/kg body weight for 1 week then taper over 3 weeks) or subconjunctival steroids necessary if no improvement after 3 days
- +/- local cycloplegics like Atropine gtt
- +/- Ciclosporin 0.05% gtt
{kind=link}
{kind=link}
Treatment Regimen after Corneal Transplantations (PKP, DSAEK, DMEK)
Possible regimen; preparations/dosages may vary depending on clinic/surgeon
- 1st Week: Pred forte eye drops 2 hourly, Ultracortenol eye ointment at night, Floxal eye drops 3x per day for 1 week then stop
- 2nd-4th Week: Pred forte eye drops 4x per day, Ultracortenol eye ointment at night
- After 1 Month: Pred forte eye drops 3x per day and Ultracortenol eye ointment at night
- After 3 Months: Dexafree UD 3x per day and Ultracortenol eye ointment at night
- After 6 Months: Dexafree UD 2x per day
- After 9 Months: Dexafree UD 1x per day
- After 12 Months: FML Liquifilm eye drops 1x per day long term, if no pressure problems
Follow-up:
- 1st Month: Approximately weekly checks (Epithelial closure? IOP? Adherent lamella?)
- After 1 Month: Possibly suturolisis of scleral suture depending on astigmatism
- From 2nd to 6th Month: Monthly checks
- After 6 Months: Approximately every 3 months
- After 1 Year: Approximately every 6 to 12 months
- Confocal microscopy (endothelial cell count?) every 3-6 months during the first year, then every 1-2 years
Sources
- Blaubuch Augenklinik Luzerner Kantonsspital
- EyeWiki Penetrating Keratoplasty
- EyeWiki DALK
- EyeWiki Descemet’s stripping endothelial keratoplasty
- EyeWiki Descemet Membrane Endothelial Keratoplasty
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Kalla Gervasio MD, Travis Peck MD et al; Lippincott Williams&Wilkins; 8th Edition (2021)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; John E Salmon MD; Elsevier; 9th Edition (2019)