Change Language German
Emergency Treatment
- Very brief medical history: accident with lime plaster, spray plaster or similar?
- Remove the material from the eye and from under the eyelids (double evert upper eyelids)
- Intensive irrigation until pH is within the normal range (7-7.5)
- Topical anesthesia with Tetracaine gtt
- Diphotherine 500ml for severe burns
- BSS 500ml / Ringer 500ml for mild burns (e.g., mild spray injuries with hairspray or window cleaner)
- After irrigation, examine with a slit lamp.
- Visual acuity, IOP
- Assess the extent of burns:
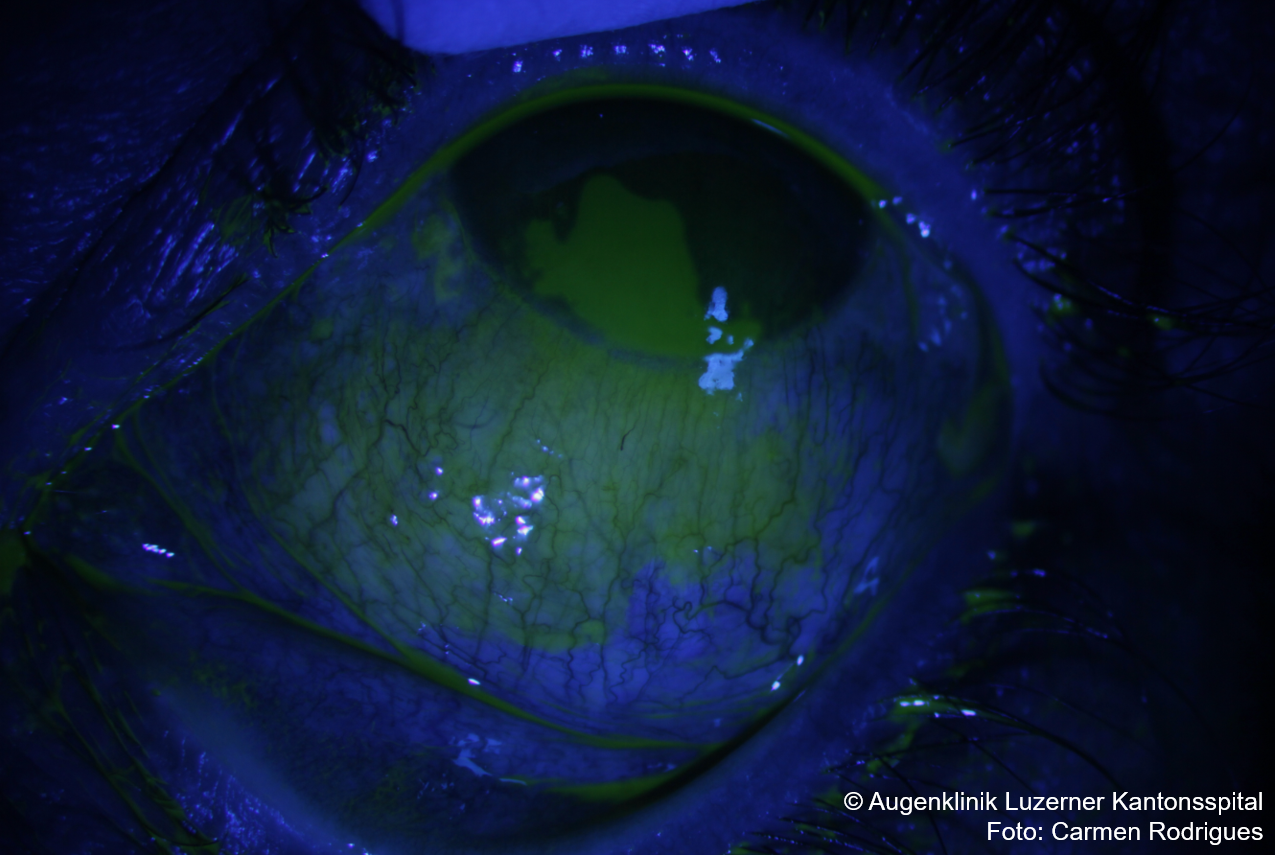
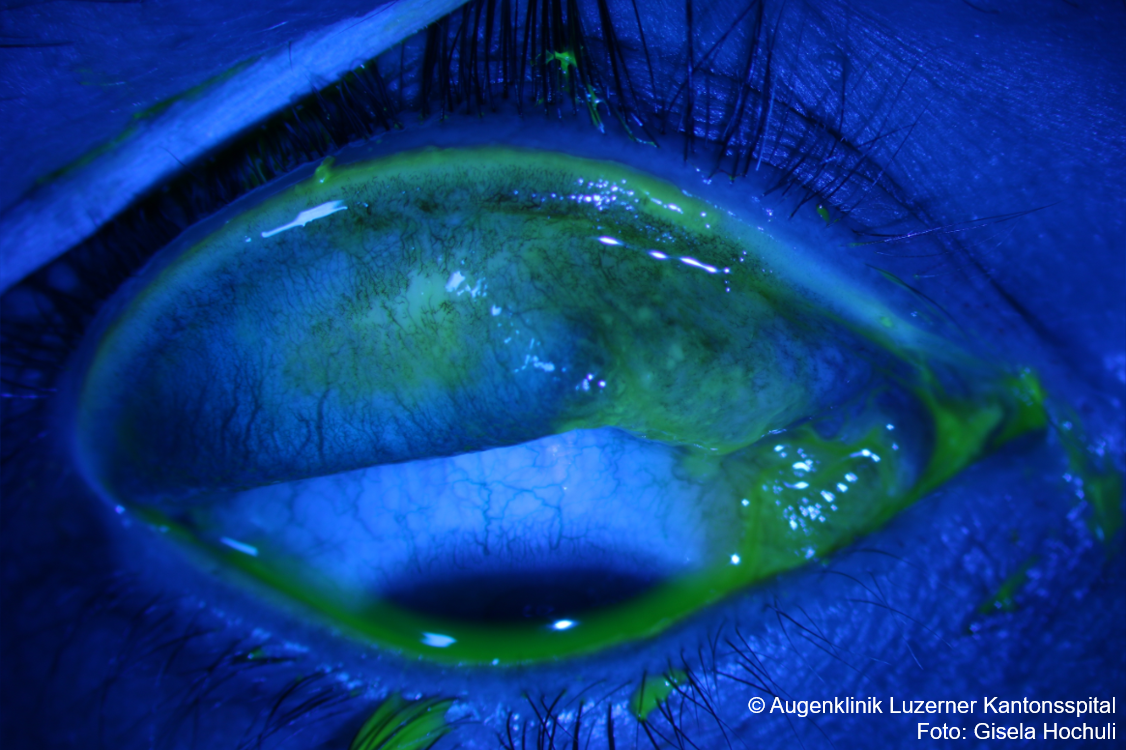
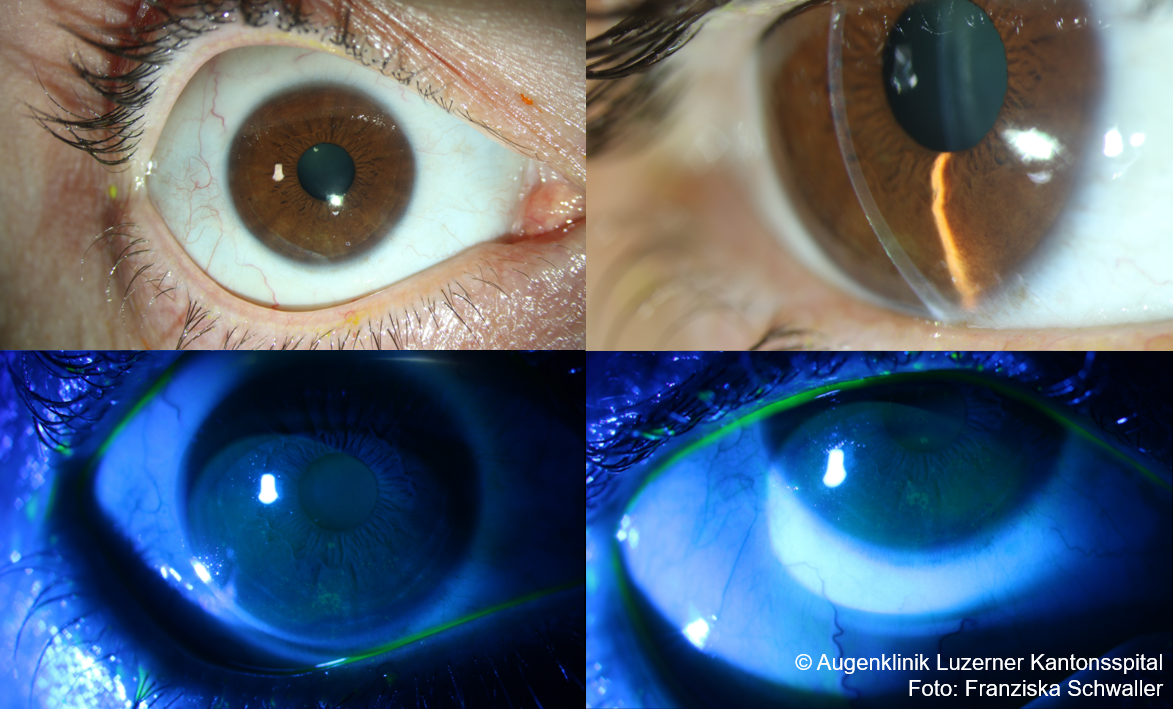
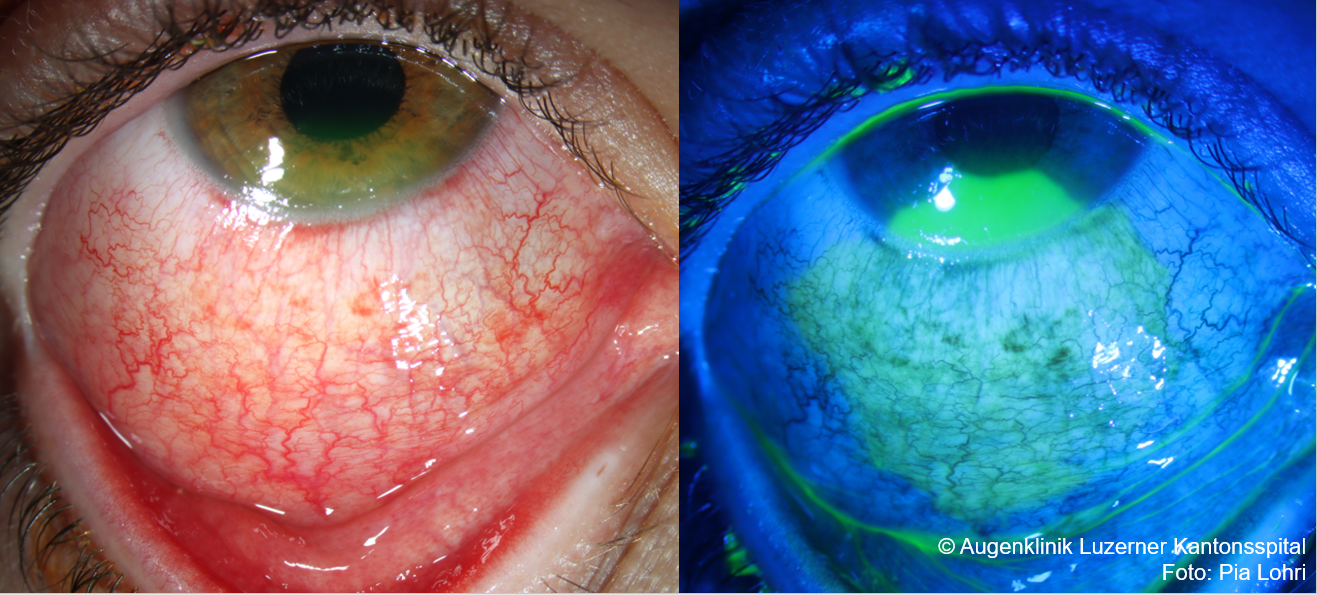
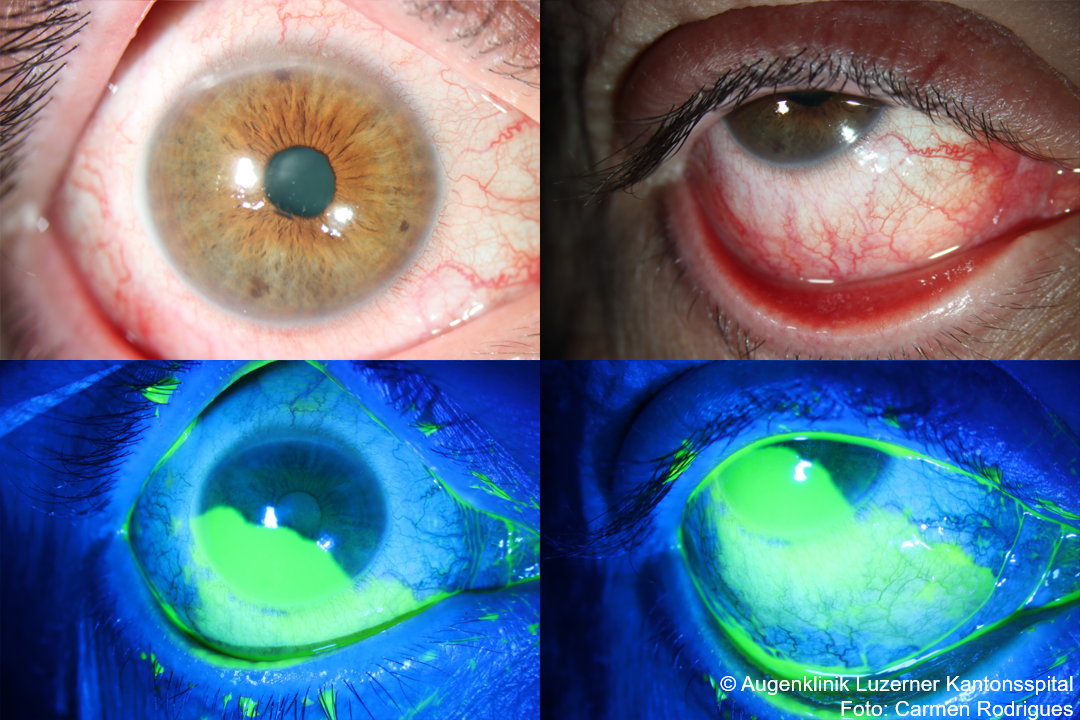
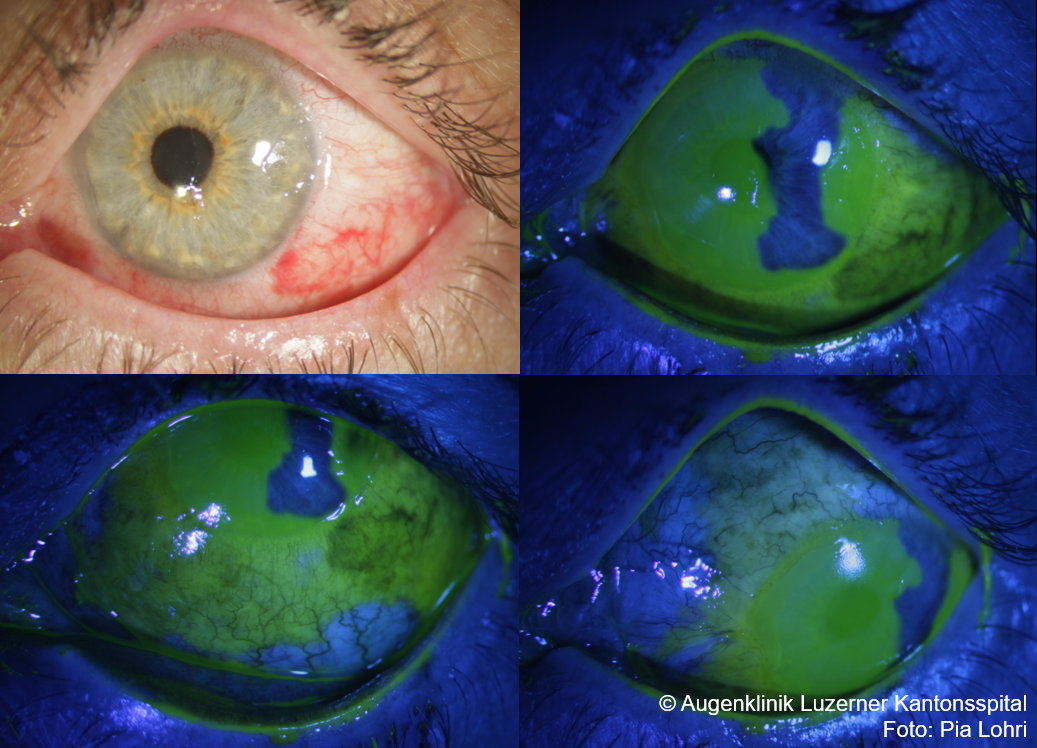
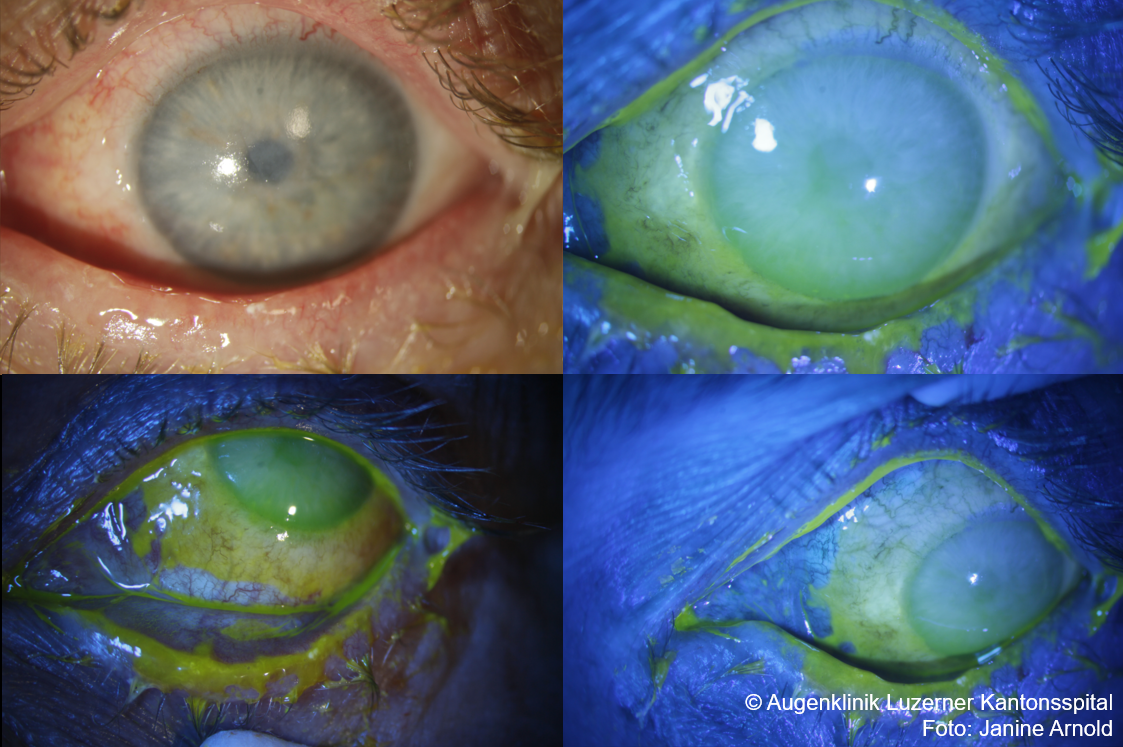
- Extension of limbal damage (fluorescein-staining) over how many clock hours?
- intact perilimbal capillary network (compare with the opposite eye)?
- Conjunctival involvement? (fluorescein-staining, typically less bright than corneal staining)
- Corneal epithelial defect? Corneal opacity? Perforation? Stromal edema? Descemet folds?
- Extension of limbal damage (fluorescein-staining) over how many clock hours?
- Measure pH again (wait about 10 minutes after irrigation)
- If pathological: continue irrigation until pH is normal + symmetrical
{kind=link}
{kind=link}
Classification
- Dua Classification
- Limbal damage: fluorescein-staining conjunctiva at the limbus?
- Conjunctival involvement (staining): bulbar conjunctiva up to/with fornix; tarsal conjunctiva is not counted
- The stage can change during follow-up: reevaluation in follow-up examinations
- Corneal epithelial defect is not a criterion for the Dua classification
- Examples:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

- Roper Hall Classification (older)
- Limbal ischemia: Evaluate the perilimbal capillary network: intact?
- Conjunctival staining is not a criterion for classification
{kind=link}
Treatment for mild burns (Dua I-II, outpatient)
- Emergency treatment with intensive irrigation until pH is normal (7-7.5) (see above)
- Lacrycon gtt 1-2 hourly during the day (or other preservative-free lubricating eye drops)
- Floxal (ofloxacin) UD 4x/day + Dexafree (dexamethasone) UD 4x/day
- Alternatively, Tobradex (tobramycin) gtt 4x/day (CAUTION: Preservatives!)
- Pain Management
- e.g., Paracetamol (4x500mg/day) or Ibuprofen (3x400mg/day)
- Additionally, cycloplegics (e.g., Cyclogyl (cyclopentolate) 1% gtt 2-3x/day)
- CAUTION: No phenylephrine due to vasoconstriction
- If elevated intraocular pressure: Diamox 250mg 3×1/day, possibly Timolol 0.5% gtt 2x/day (preservative-free)
- CAUTION: No alpha-agonists due to vasoconstriction
Therapy for moderate to severe burns (Dua III-VI, hospitalisation)
- Emergency treatment with intensive irrigation until pH is normal (7-7.5) (see above)
- Then, continue irrigation with BSS every half-hour for at least 3 hours
- Remove necrotic tissue
- Lacrycon gtt (or other lubricating eye drops) hourly during the day
- Floxal (ofloxacin) UD 4x/day
- Dexafree (dexamethasone) UD or Pred Forte (prednisolone) gtt 1-2 hourly
- Pain Management
- e.g., Paracetamol (4x500mg/day) or Ibuprofen (3x400mg/day)
- Additionally, cycloplegics (e.g., Cyclogyl (cyclopentolate) 1% gtt 2-3x/day)
- CAUTION: No phenylephrine due to vasoconstriction
- If elevated intraocular pressure: Diamox 250mg 3×1/day, possibly Timolol 0.5% gtt 2x/day (preservative-free)
- CAUTION: No alpha-agonists due to vasoconstriction
- Additional therapy options:
- Doxycycline 100mg p.o. 1x/day for 2 weeks
- Vitamin C p.o. (e.g., Redoxon effervescent tablets 1g 2x/day) for 2 weeks
- Sodium Citrate 10% gtt 4-6x/day for 2 weeks
- CAUTION: Causes strong burning
- Autologous serum eye drops (undiluted)
- Symblepharon prophylaxis for tarsal conjunctival involvement: Sweep the fornix with a glass spatula and Floxal ointment 1-2x/day
- Depending on the course: Amniotic membrane , tarsorrhaphy, limbal stem cell transplantation
{kind=link}
Sources
- Dr. med. Philippe Bänninger, Schwere Augenverätzungen, Blaubuch Augenklinik Luzerner Kantonsspital
- EyeWiki Chemical Injury of Conjunctiva and Cornea
- Dua HS, King AJ, Joseph A. A new classification of ocular surface burns. Br J Ophthalmol. 2001;85(11):1379-1383. doi:10.1136/bjo.85.11.1379
- Roper-Hall MJ. Thermal and chemical burns. Trans Ophthalmol Soc U K. 1965;85:631-53. PMID: 5227208.
- Baradaran-Rafii A, Eslani M, Haq Z, Shirzadeh E, Huvard MJ, Djalilian AR. Current and Upcoming Therapies for Ocular Surface Chemical Injuries. Ocul Surf. 2017;15(1):48-64. doi:10.1016/j.jtos.2016.09.002
- Bizrah, M., Yusuf, A. & Ahmad, S. An update on chemical eye burns. Eye 33, 1362–1377 (2019). https://doi.org/10.1038/s41433-019-0456-5
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition(2015)