Change Language German
Types
- Branch Retinal Vein Occlusion (BRVO) vs. Central Retinal Vein Occlusion (CRVO)
{kind=link}
{kind=link}
Risk Factors
- Cardiovascular risk factors: Age > 60 years, cardiovascular disease, hypertension, obesity, nicotine abuse, diabetes mellitus (not a risk factor in BRVO)
- Ocular: Glaucoma, optic disc drusen, increased intraorbital and/or intraocular pressure
- Others: Syphilis, sarcoidosis, vasculitis, hyperviscosity syndromes (multiple myeloma, leukemia, Waldenström’s macroglobulinemia), sickle cell disease, HIV, hyperhomocysteinemia, elevated ESR, oral contraception
Findings
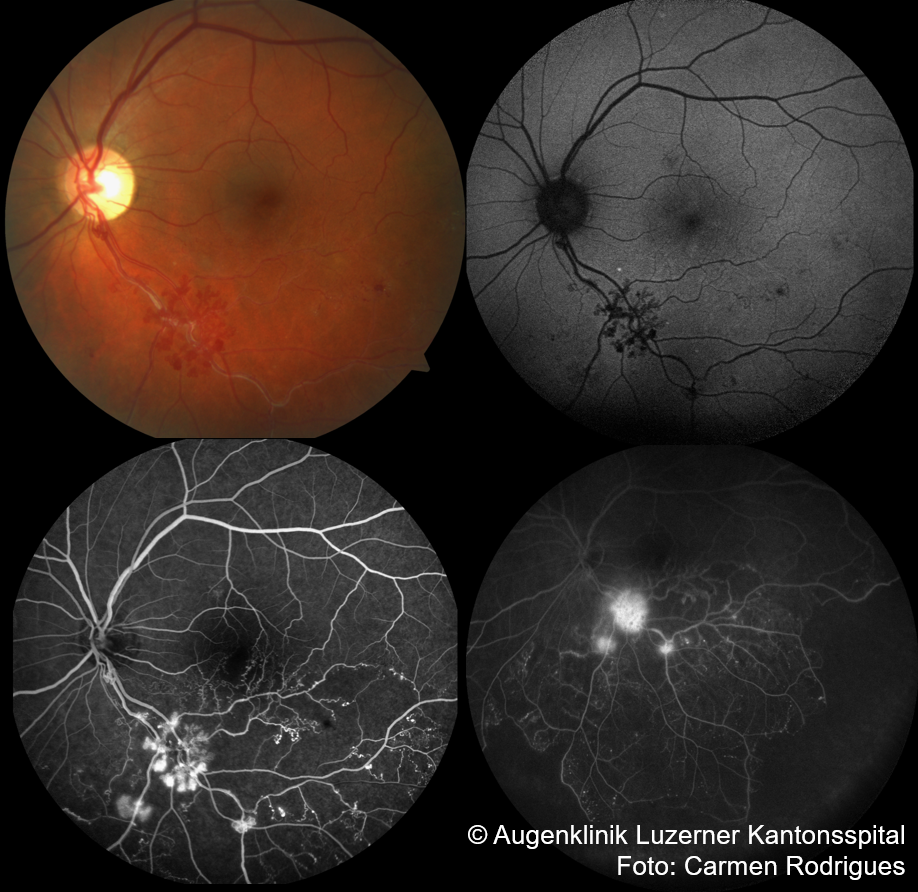
- Dot/blot and flame-shaped hemorrhages in all quadrants (CRVO) or along the branch vein
- (BRVO; mostly superotemporal)
- Dilated, tortuous vessels , optic disc swelling (in CRVO) , macular edema
- Possible cotton-wool spots, hard exudates, retinal edema
- Neovascularisations if ischemic (iris , chamber angle , optic disc, retina ), neovascular glaucoma (“90-day glaucoma”)
- Visual field defects, central scotoma in macular BRVO
- Over time: shunt vessels, microaneurysms, sclerosed vessels, telangiectasia
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Work-up
- Clinical examination
- Evaluation of cardiovascular / haematological risk factors:
- Blood pressure
- Laboratory: complete blood count, CRP, ESR, glucose, HbA1c, lipid profile, Quick/INR
- In patients < 50 years, consider haemotological assessment
- Further evaluations by primary care physician: e.g., ECG, 24h blood pressure monitoring, carotid duplex sonography (rule out ocular ischemic syndrome)
- OCT: Macular edema?
- Rule out glaucoma: IOP measurement
- Fluorescein angiography after resorption of hemorrhages (after approx. 4 – 6 weeks, at the latest after 3 months): extent of ischemic areas? ischemic vs. non-ischemic
Treatment
- Macular edema: anti-VEGF therapy; alternatively intravitreal steroids
- IOP reduction (even with only slightly elevated pressure)
- Retinal photocoagulation:
- For neovascularisations of the iris, angle, optic disc, or retina (according to Central Vein Occlusion Study CVOS), possibly additional temporary anti-VEGF therapy
- Depending on clinical findings: consider initial prophylactic treatment for ischemic CRVO/BRVO
- Consider cyclophotocoagulation for secondary glaucoma
- Hemodilution controversial!
Follow-up
- In the first 6 months: monthly follow-up controls, including gonioscopy (if clearly non-ischemic, follow-up control also possible after 3 months)
- Neovascularisations in about 60% of ischemic CRVO, mostly within 2-4 months -> “100-day glaucoma”
- Conversion from non-ischemic to ischemic CRVO: about 16%
- In the first two years: follow-up controls at 3-6 month intervals due to the risk of neovascularisation
Sources
- EyeWiki Central Retinal Vein Occlusion
- EyeWiki Branch Retinal Vein Occlusion
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Kalla Gervasio MD, Travis Peck MD et al; Lippincott Williams&Wilkins; 8th Edition (2021)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; John E Salmon MD; Elsevier; 9th Edition (2019)
- Review of Ophthalmology; Autoren/Verlag: Neil J. Friedman MD, Peter K. Kaiser MD, William B. Trattler MD; Elsevier; 3rd Edition (2017)