Change Language German
Most Common Causes
- Atherosclerosis: Occlusion at the level of the lamina cribrosa in central retinal artery occlusion (CRAO)
- Emboli: carotid artery, calcified heart valves, cardiac thrombus
- Vasculitis: Giant cell arteritis
Findings
- History (emboli or arteritis)
- Check pupils, relative afferent pupillary defect (RAPD)
- Visual acuity (often only counting fingers)
- Fundus examination in miosis, compare bilaterally (initial mydriasis not required)
- Inspection and palpation of the temporal artery: temporal arteritis?
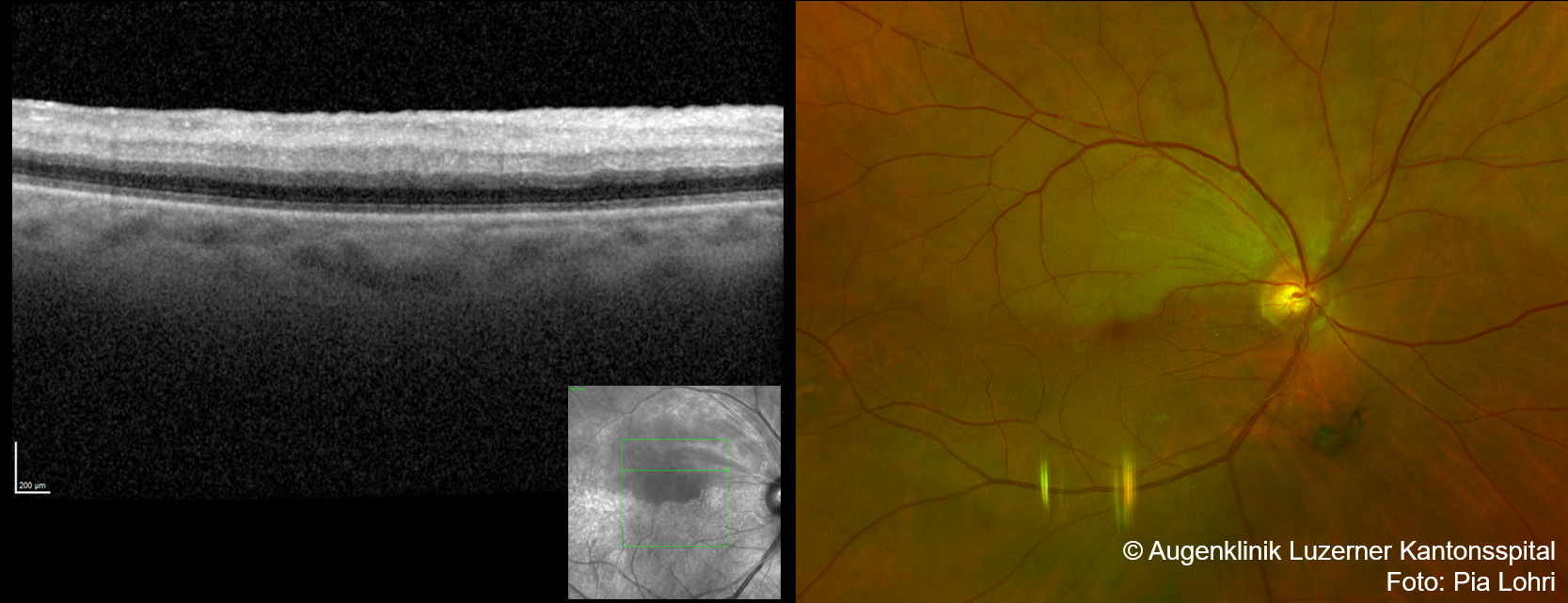
- OCT: hyper-reflective inner retinal layers
{kind=link}
{kind=link}
{kind=link}
Work-up
- Laboratory tests (blood count, CRP, ESR) if suspected giant cell arteriitis or to rule out in patients >50 years
- Referral to Stroke Unit/Neurology for further assessment (stroke work-up)
- Prescribe 100mg/d aspirin after consultation with the neurologist
- In patients < 50 years, in addition to TTE and 24h ECG: consider screening for thrombophilia and vasculitis
- If suspected arteritic origin –> Plan duplex sonography of extracranial vessels and temporal artery biopsy
Acute Phase Treatment
Note: No recognized treatment regimen, as there is no clear data, no obligation for treatment (except for arteritic origin)
- Ocular massage for 3-5 minutes with 3-mirror contact lens or digital massage (can also be performed by patient)
- Consider reducing intraocular pressure with Diamox 500mg i.v. + topical Timolol 0.5% gtt
- Paracentesis is not recommended
- Consider intravenous fibrinolysis, up to 4.5 hours after the onset
- For suspected arteritic origin: hospitalisation and treatment with high-dose steroids
Follow-up
- After 2, 4, 8, and 24 weeks, possibly more frequently
- Fluorescein angiography not mandatory but helpful for detecting neovascularisation and assessing perfusion
Prognosis
- Generally poor, with most patients having permanently reduced visual acuity (< 0.05)
- Spontaneous improvement in vision in 1-8% of patients, typically in cases involving the cilioretinal artery
- <5% develop neovascular glaucoma
Sources
- AWMF Leitlinie Retinale Arterienverschlüsse
- EyeWiki Retinal Artery Occlusion
- EyeWiki Branch Retinal Artery Occlusion
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition(2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)