Change Language German
Important Forms of Age-Related Cataract
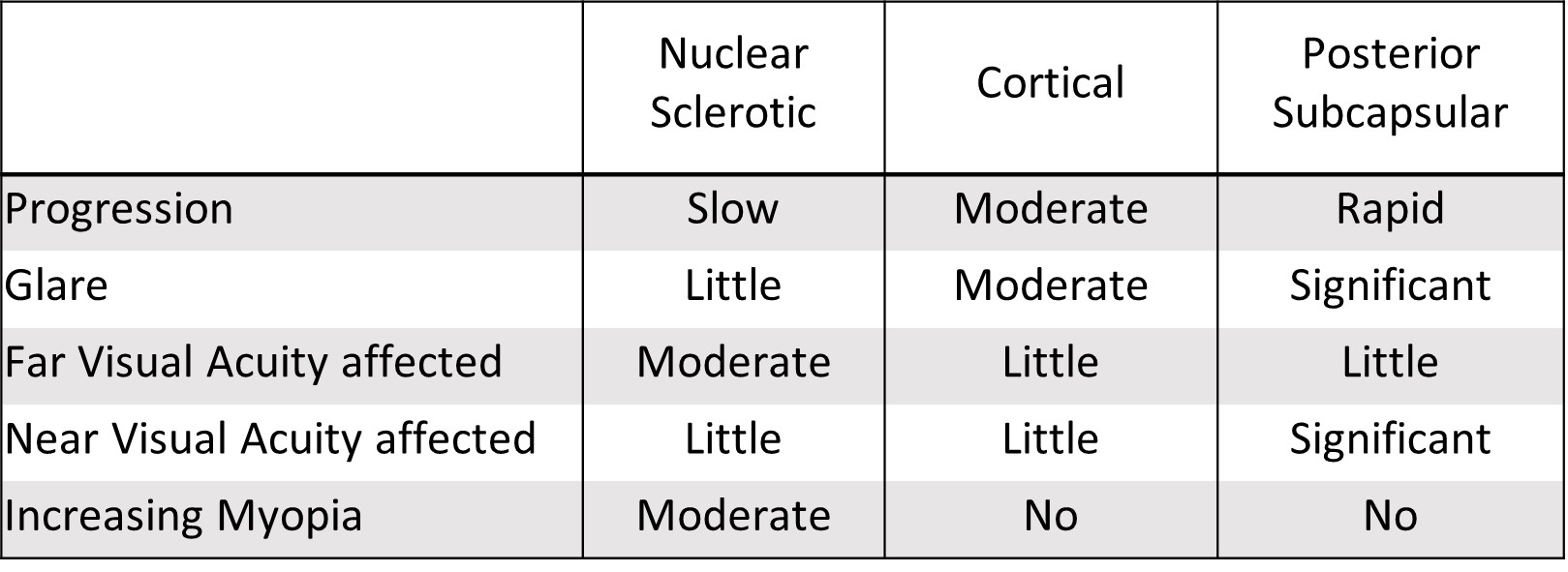
- Overview of symptoms
- Nuclear Sclerotic
- Cortical
- Can affect anterior, posterior, or equatorial cortex
- Initial fissures and vacuoles, then typical wedge-shaped or radial, spoke-like opacities
- Often causes glare
- Posterior Capsular Opacification
- Well-visible in retroillumination
- Opacity located directly in front of the posterior capsule
- Vacuolated, granular, or plaque-like appearance
- Often causes glare
{kind=link}
{kind=link}
Stages
- Immature Cataract: Lens partially opacified
- Mature Cataract: Lens completely opacified
- Hypermature Cataract: Shrunken and wrinkled capsule due to water leakage from the lens
- Morgagnian Cataract: Hypermature cataract where liquefaction of the cortex causes the nucleus to sink downward
Risk Factors
- Steroid therapy, trauma, UV light, smoking, diabetes, myopia
Postoperative Follow-up Day 1
- Visual acuity not obligatory
- Corneal edema?
- Anterior chamber:
- Deep? If shallow: Seidel test
- Cells/flare/fibrin/blood/hypopyon?
- IOL positioned correctly? Is the posterior capsule intact?
- Round/distorted pupil? If teardrop-shaped: Vitreous in the anterior chamber?
- IOP
- < 5mmHg: Seidel test
- If anterior chamber is shallow and Seidel test positive -> Bandage contact lens (16mm diameter), Floxal UD 4x/d, Dexafree 4x/d, follow-up after 1-2 days
- If anterior chamber is collapsed: Inform senior physician/surgeon
- 5 – 25mmHg: Treatment and follow-up as planned
- 26 – 35mmHg: Lower IOP
- Known glaucoma and glaucoma drops not taken yet: Re-administer own glaucoma drops first, follow-up after 1-2 days
- No known glaucoma: Diamox 250mg 2×1 tbl./d, follow-up after 1-2 days
- >35mmHg: Inform senior physician/surgeon
- Viscoelastic in anterior chamber? (little/no convection)
- Consider releasing pressure via paracentesis
- Viscoelastic in anterior chamber? (little/no convection)
- < 5mmHg: Seidel test
- Retinal examination only if symptoms of detachment
Postoperative Complications
- Increased IOP (see above)
- Wound leakage (see above)
- IOL (Sub-)luxation
- Posterior capsule opacification (“second cataract”)
- Toxic Anterior Segment Syndrome (TASS)
- within 24 hours postoperatively!
- Endophthalmitis
- Corneal edema
- IOP decompensation? Endothelial defect? Fuchs endothelial dystrophy?
- Macular edema (Irvine-Gass syndrome?)
- Retinal detachment
- Ptosis
- Expulsive suprachoroidal haemorrhage
- very rare, acute severe pain, loss of vision, IOP increased, +/- shallow anterior chamber
Sources
- EyeWiki Cataract
- EyeWiki Morgagnian Cataract
- EyeWiki Cataract Surgery Complications
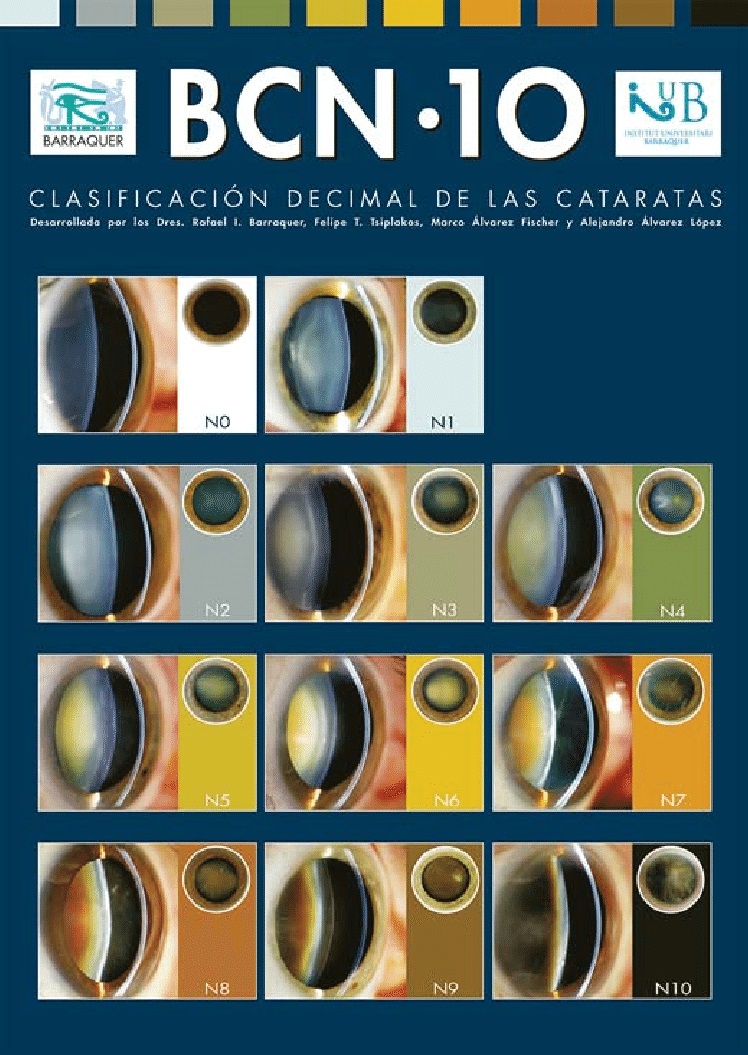
- ¹Barraquer R, I, Pinilla Cortés L, Allende M, J, Montenegro G, A, Ivankovic B, D’Antin J, C, Martínez Osorio H, Michael R: Validation of the Nuclear Cataract Grading System BCN 10. Ophthalmic Res 2017;57:247-251. doi: 10.1159/000456720
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)