Change Language German
General
- if cells / bleeding in anterior chamber = blunt trauma with traumatic iritis
- if no cells in anterior chamber: probably no direct bulbar trauma
Initial Examination
- Corneal lesion?
- Conjunctival lesion? Any sign of penetration?
- Asymmetric anterior chamber? Asymmetric IOP? Seidel?
- Cells in anterior chamber / iritis?
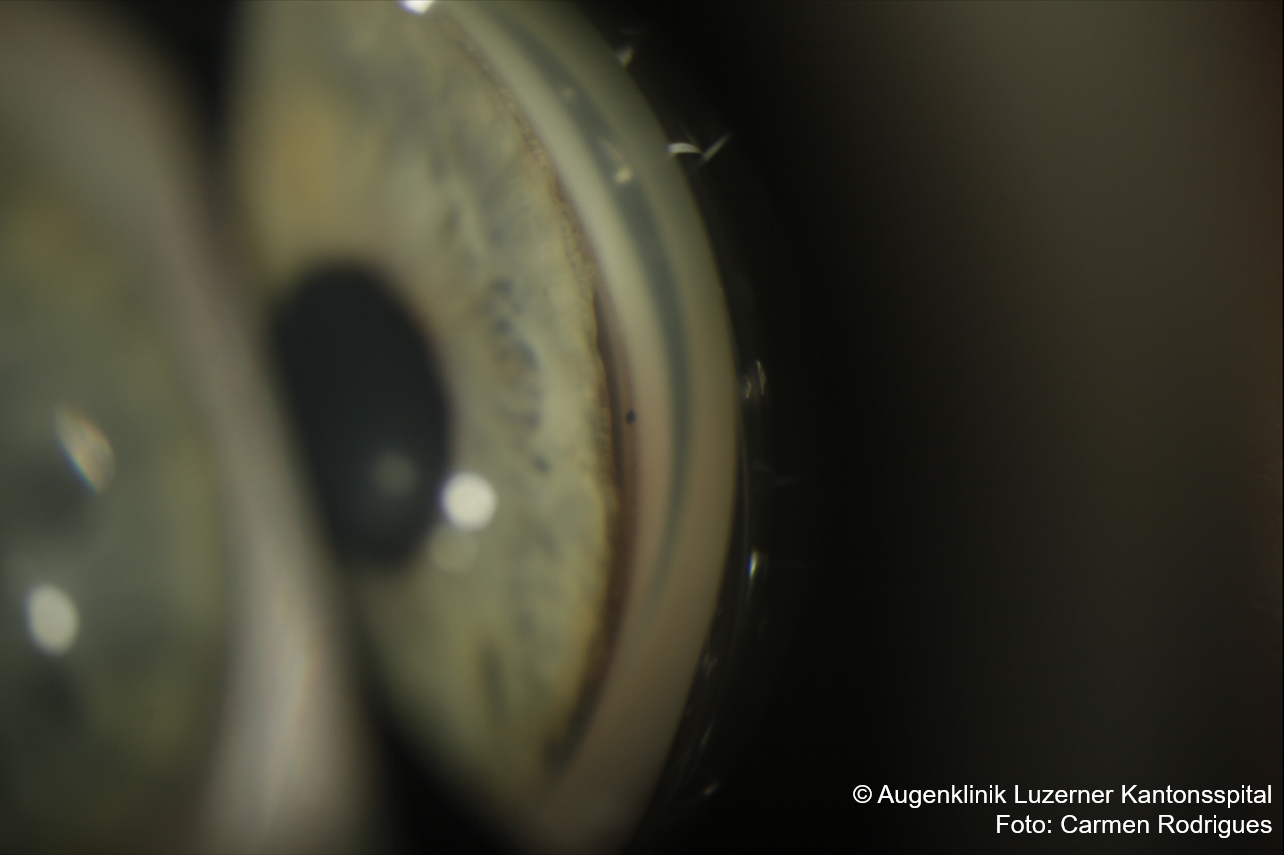
- Hyphaema?
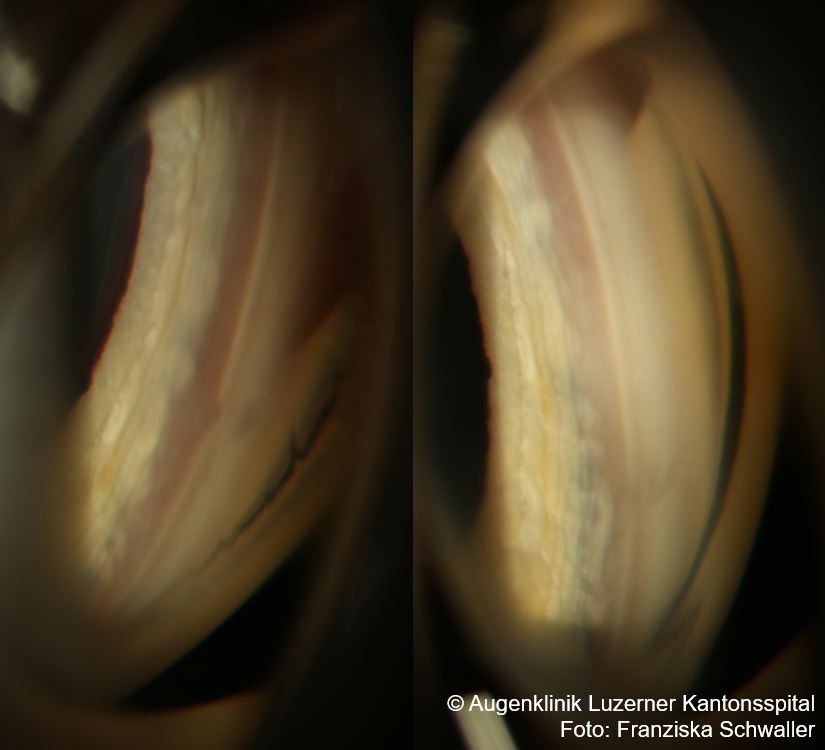
- Gonioscopy once bleeding is dissolved (Caution: Risk of rebleeding!)
- Screening for sickle cell anaemia in black patients
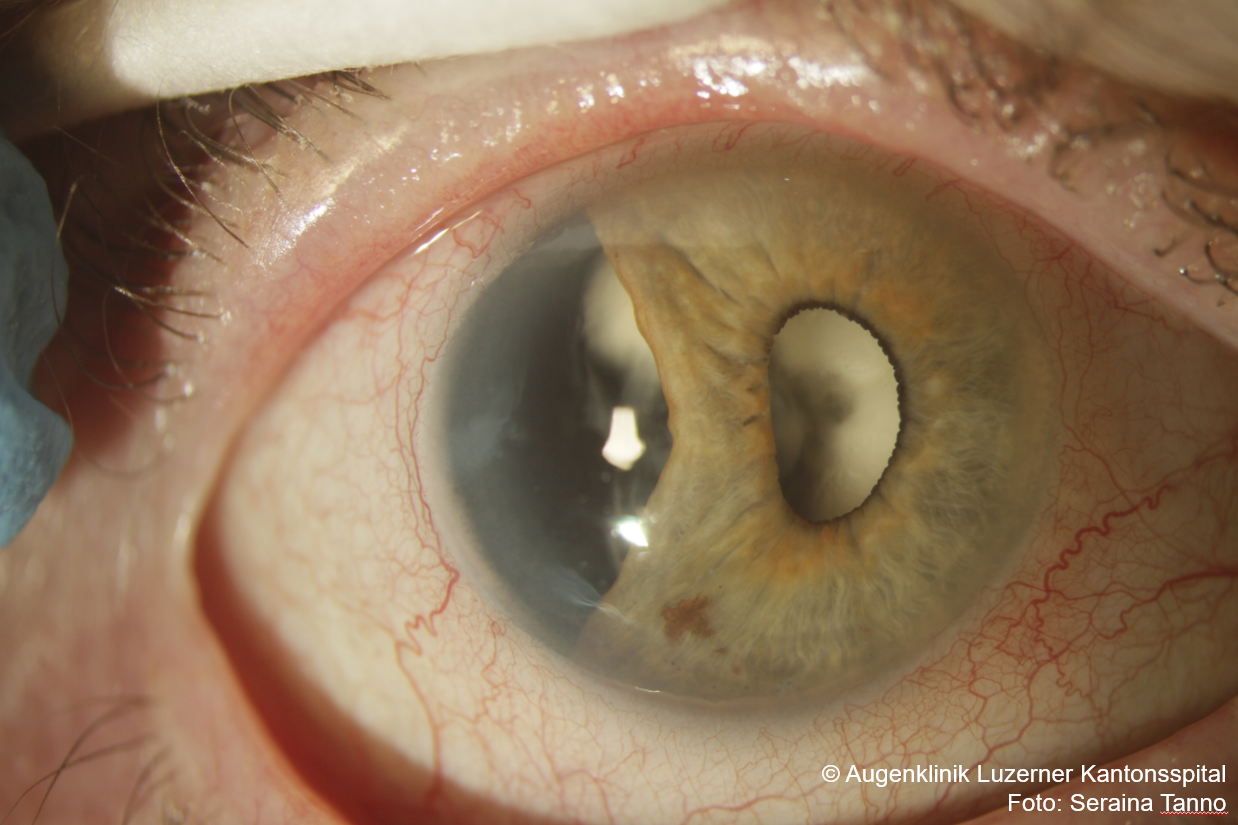
- Traumatic mydriasis? Iridodialysis?
- IOP?
- If retinal tear/detachment is suspected, perform dilated funduscopy
- Palpate orbital rim, check ocular motility and skin sensitivity (lower eyelid to upper lip) -> Signs of orbital fracture?
{kind=link}
Therapy
- Start with topical steroids in case of anterior chamber cells
- e.g. Pred forte gtt (Prednisolon) or Dexafree SDU (Dexamethason) 4x daily to hourly
- Alternatively Yellox gtt (Bromfenac) 3x daily for 1-2 weeks
- consider additional Voltaren 50mg p.o. (Diclofenac) 3x daily for 3-5 days
- Taper quickly depending on anterior chamber cells.
- e.g. Pred forte gtt (Prednisolon) or Dexafree SDU (Dexamethason) 4x daily to hourly
- In case of conjunctival / corneal injury, use antibiotic drops
- e.g. Floxal gtt (Ofloxacin) 4x/d.
- In case of increased IOP
- e.g. Cosopt gtt (Dorzolamid+Timolol) 2x/d (caution: asthma, sickle cell disease)
- Alternatively Diamox 250mg p.o. (Acetazolamid) max. 3×1 tbl./d (caution: sickle cell anaemia)
- If no signs of retinal complications (e.g. retinal detachment, Berlin oedema ) -> Dilated fundoscopy after ca. 1 week, otherwise at first presentation.
- Inform patients about warning signs of retinal detachment!
{kind=link}
Follow-up
- after 1-2 days depending on severity -> measure IOP
- Always after 5-7 days: dilated fundoscopy
- Gonioscopy if anterior chamber angle recession is suspected
- Hyphaema? Recession probable, gonioscopy once completely reabsorbed
- Severe blunt trauma
- If recession >180°: significantly increased lifelong risk of developing glaucoma -> annual follow-ups
- IOP control after approx. 2 weeks: Steroid responder?
- Check after 1 month with gonioscopy and dilated fundus examination
- Follow-up with fundus examination and IOP control after 3-6 months, then annually.
- In case of recession >180°: lifelong recommended
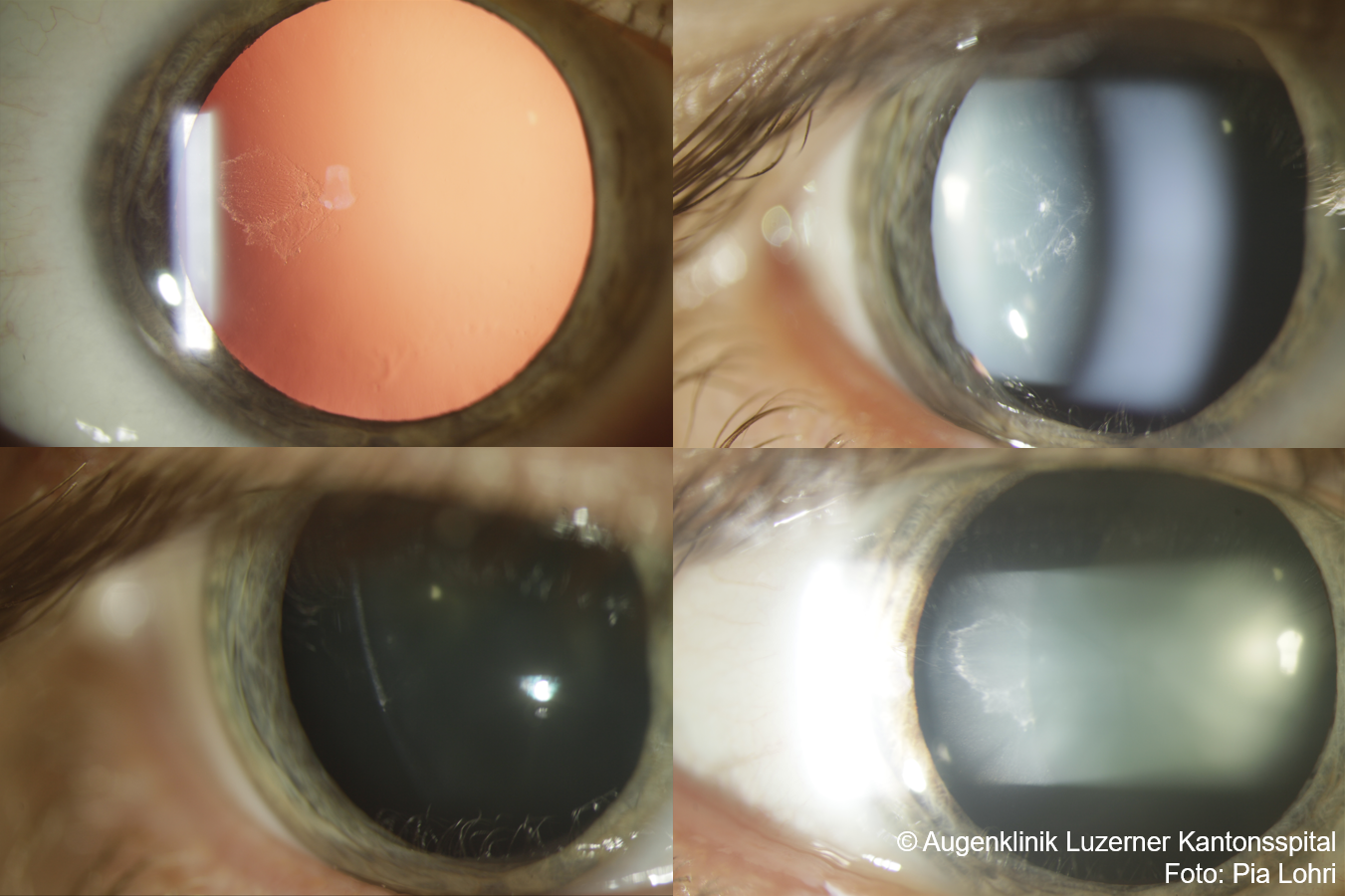
- Information about risk of traumatic cataract, retinal detachment, secondary glaucoma
{kind=link}
{kind=link}
{kind=link}
Sources
- EyeWiki Ocular Trauma
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)