Change Language German
Aetiology
- Common pathogens
- Staph. aureus, Streptococci (S. pyogenes, S. pneumoniae)
- Pseudomonas (frequent in contact lens wearer)
- Pathogens that can penetrate intact corneal epithelium
- N. gonorrhoeae, N. meningitidis, C. diphtheriae, H. influenzae
Risk Factors
- Contact lens wear (especially long wearing time, soft contact lenses, poor lens hygiene)
- Trauma
- Ocular surface diseases (herpes keratitis, dry eye, chronic blepharitis…)
- Local or systemic immunosuppressants
- Diabetes mellitus
- Vitamin A deficiency
Workup
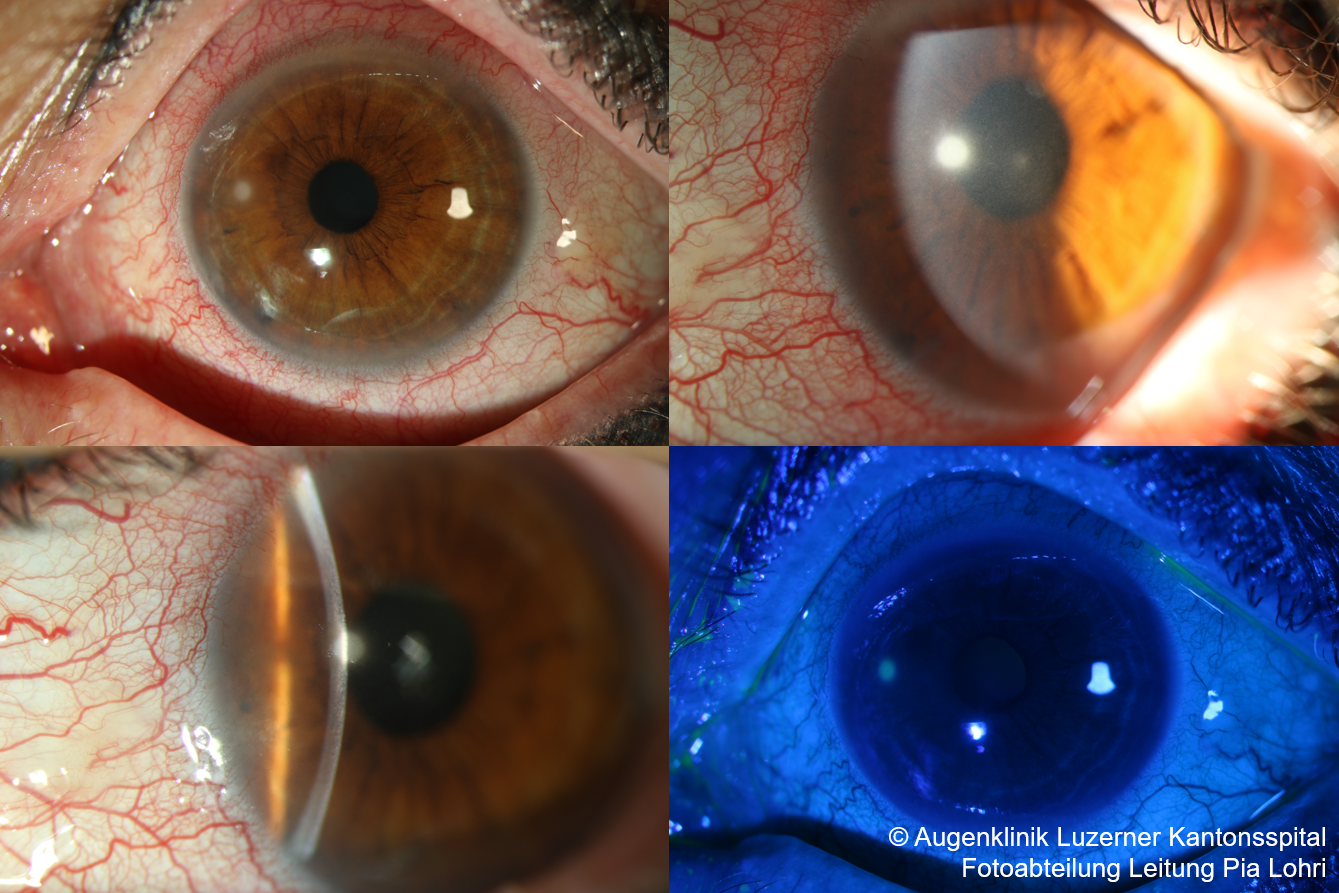
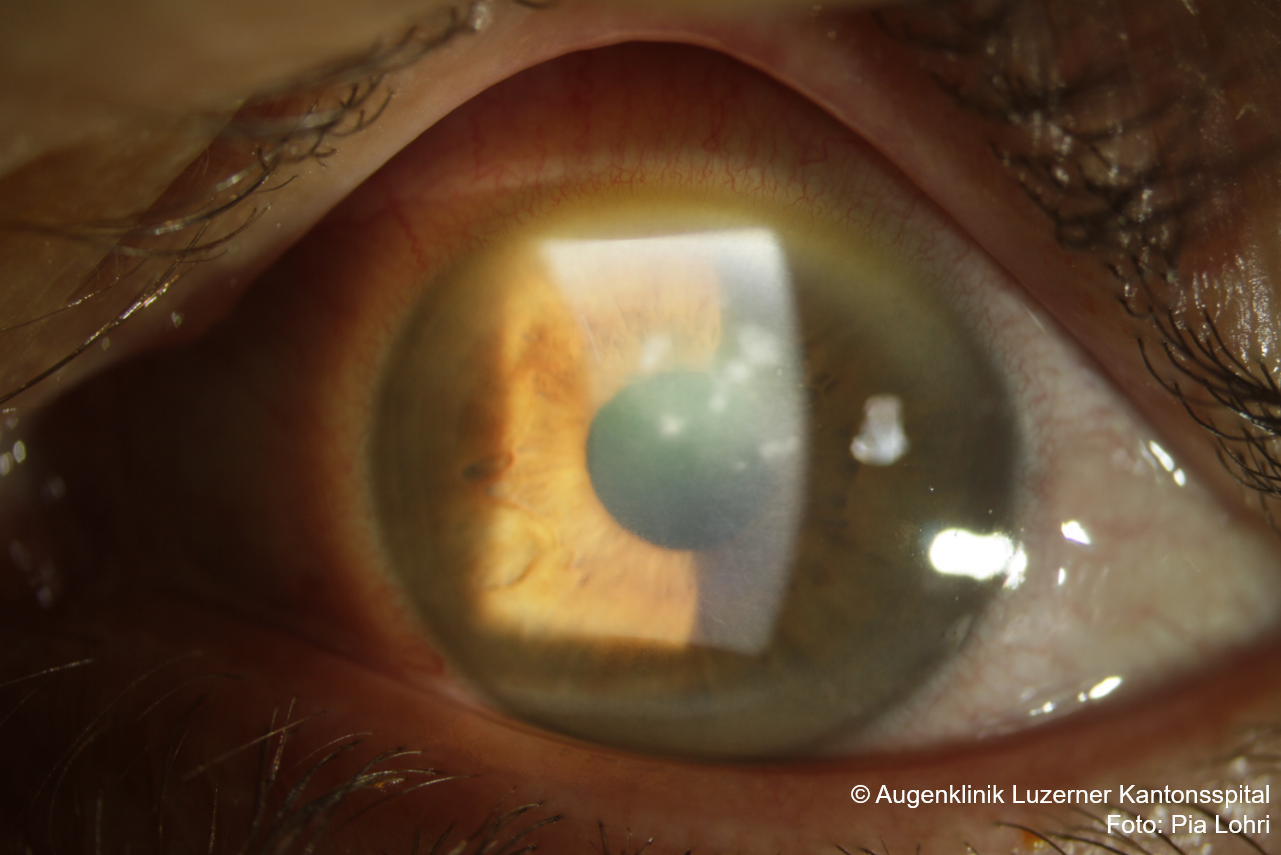
- Photo documentation
- Specimen collection in case of
- Infiltrate >1mm or affecting central visual axis or no response to initial therapy
- In case of non-central infiltrate <1mm: Smear not mandatory due to only small probability of germ detection
- Optimal: direct preparation, culture for bacteria + fungi, consider viral PCR (HSV, VZV)
- Consider sending in contact lens container including contact lens to microbiology
- Especially if acanthamoebae are suspected, otherwise not very helpful, as containers are always contaminated
{kind=link}
Management
- Infiltrate size < 1mm:
- Floxal gtt (Ofloxacin) 5x/d to hourly and Floxal ointment at night
- Infiltrate size > 1mm:
- Ceftazidim/Ofloxacin gtt hourly in the first 24 – 48h, thereafter, depending on response, reduce frequency during the day and switch to Floxal ointment at night
- Large/multiple infiltrates :
- Cefta/Ofloxacin gtt initially every 15min (in the first 2-3h for rapid saturation), then hourly as described above
- Consider inpatient admission depending on the size of the findings, if perforation is imminent or if there are compliance problems
- Consider additional scopolamine 0.25% AT 2x/d in case of (pronounced) cell flare in the anterior chamber, (reduces ciliary spasm, pain)
- Consider additional steroids if there is a lytic process with a risk of perforation
- Systemic antibiotics usually not indicated, may be necessary e.g. in case of severe corneal thinning with imminent or acute perforation or in case of scleral involvement
- Ciprofloxacin 500mg 2x/d (good penetration into the cornea, also when administered orally)
- Systemic tetracyclines (e.g. doxycycline 100mg 2x/d) may be administered in cases of significant corneal thinning due to the anticollagenase effect
- Systemic antibiotics are indicated for potential systemic involvement in:
- N. meningitides: benzylpenicillin i.m., ceftraxone or cefotaxime or ciprofloxacin orally
- H. influenzae: oral amoxicillin with clavulanic acid
- N. gonorrhoeae: ceftriaxone (a 3rd generation cephalosporin)
- Avoid contact lens wear!
{kind=link}
Follow-up
- daily follow-ups until improvement
- Check-up after 1 day:
- Response to therapy? (Less pain? Less redness/irritation of the eyes?)
- Check-up after 2 days:
- Clinical signs of response to therapy? (Reepithelialisation? Decrease in anterior chamber cell flare? Better delineation or decrease in size of infiltrate?)
- If clinical findings show a clear improvement: Consider reducing antibiotic therapy to 2 hourly during the day, Floxal ointment at night
- If no improvement: possible causes: no response to therapy yet (too early), fungal keratitis, resistant pathogen.
- Clinical signs of response to therapy? (Reepithelialisation? Decrease in anterior chamber cell flare? Better delineation or decrease in size of infiltrate?)
- Check-up after 3-5 days:
- Consider therapy adjustment depending on culture/sensitivity report
- Decision on additional steroid therapy (no international consensus)
- Goal: Minimise scarring
- Prerequisite: confirmed diagnosis (not in fungal keratitis), confirmed clinical response to therapy with epithelialisation
- e.g. Pred Forte gtt (Prednisolone) 4x/d for one week, reduce by 1 drop every week
- Further Follow-ups depending on the course
Sources
- EyeWiki Bacterial Keratitis
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)