Change Language German
Symptoms
- Pain, redness, photophobia, tearing, possible reduction of visual acuity
Medical history
- First attack or recurrent?
- Systemic diseases/ concomitant rheumatological diseases?
- Extended medical history:
- Symptoms: Joint pain, back pain, skin lesions, discolouration/ numbness of hands and feet, diarrhoea, night sweats, fever, weight loss, dry mouth/ eyes, herpes blisters, ulcers in the mouth/ genital area.
- Other: travel history, ancestry, animals, tick bite, smoking/drinking habits, drug use, sexual history, medication, occupation, family history.
Aetiology
- Non-granulomatous
- idiopathic (approx. 50%)
- autoimmune: HLA-B27 associated: Ankylosing spondylitis (Bechterew’s disease), reactive arthritis, psoriatic arthritis, inflammatory bowel disease, Behcet’s disease (HLA-B51), juvenile rheumatoid arthritis, Kawasaki syndrome, other autoimmune diseases (lupus erythematosus, polychondritis, Wegener’s granulomatosis, interstitial nephritis)
- others: postoperative, trauma, UGH syndrome
- granulomatous
- infectious: herpes simplex virus, varicella zoster virus, syphilis, tuberculosis, leprosy, brucellosis, toxoplasmosis, propionibacterium acnes, fungi (cryptococcus, aspergillus), HIV
- Immunological: sarcoidosis, VKH syndrome, sympathetic ophthalmia, lens-associated uveitis (phacoanaphylactic uveitis).
- others: Fuchs heterochromic iridocyclitis, glaucomatocyclitic crisis (Posner-Schlossmann syndrome).
Findings
- Ciliary vascular injection
- Reactive miosis
- Anterior chamber cells / flare, fibrin, hypopyon
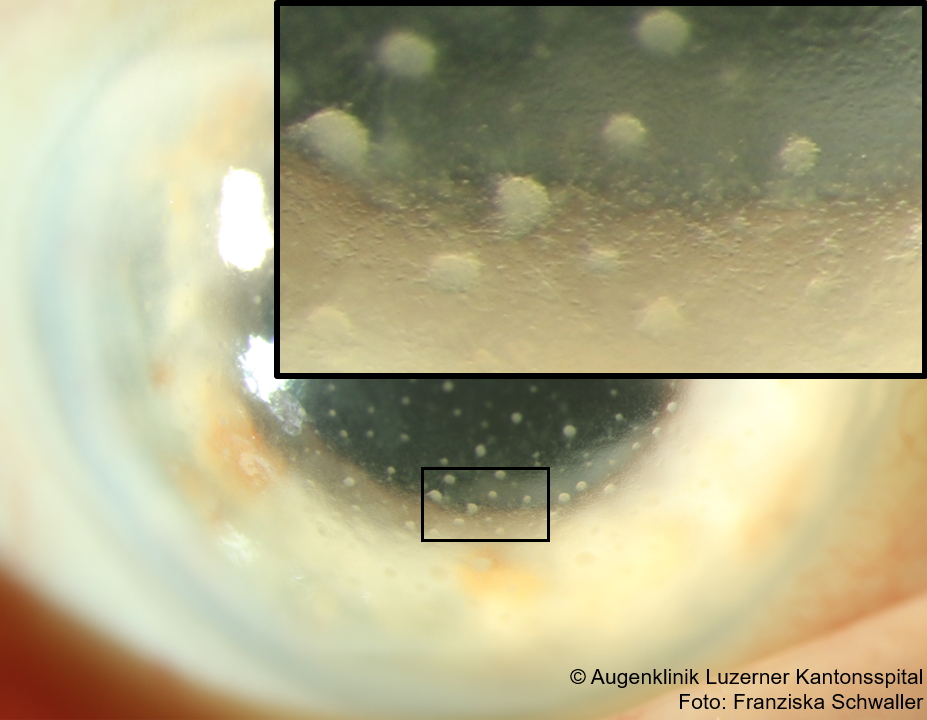
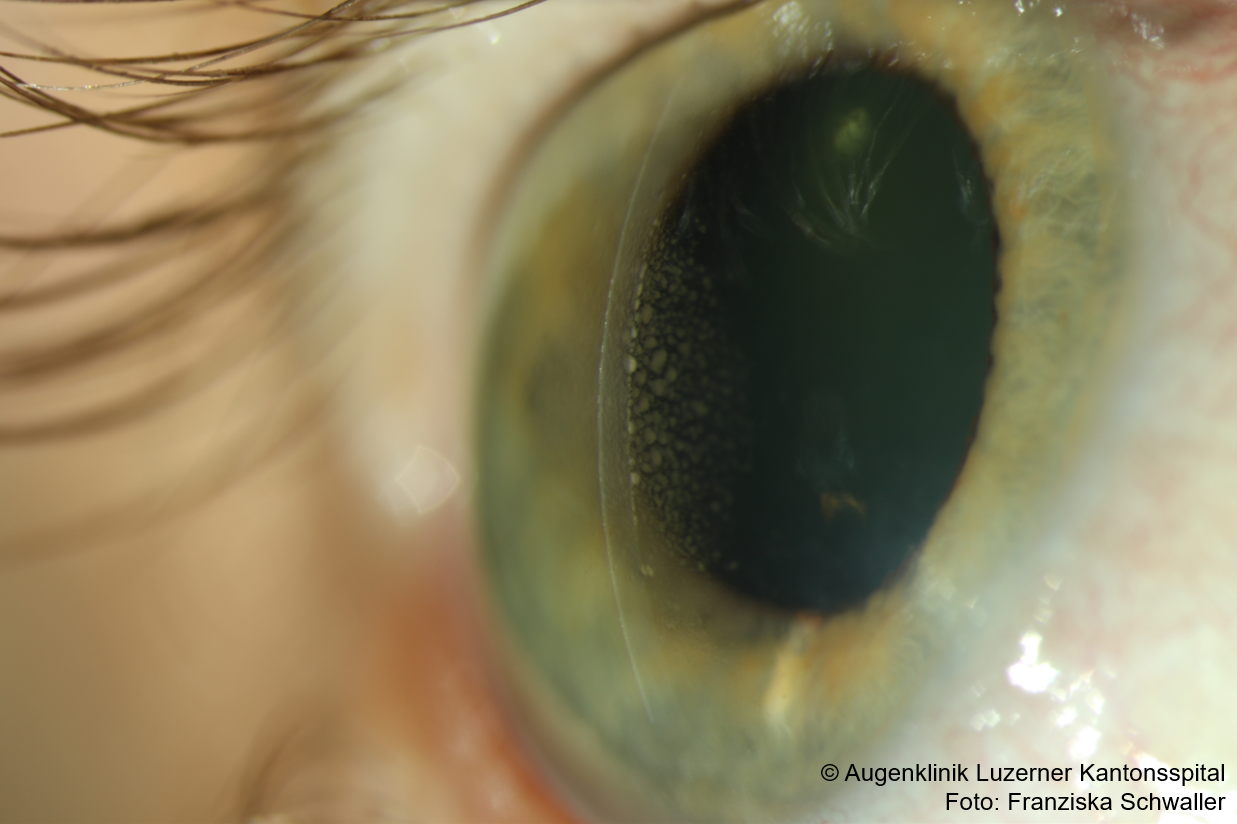
- Endothelial precipitates
- Posterior synechiae
- Iris nodules (Busacca/Koeppe), iris atrophy (diffuse, focal, segmental), heterochromia
- Vitreous cells (in case of spill-over)
- Increased intraocular pressure (-> HSV, Posner-Schlossmann, Fuchs’ heterochromic iridocyclitis)
{kind=link}
{kind=link}
{kind=link}
Examination
- Distinguish whether granulomatous or non-granulomatous
- Non-granulomatous: small, fine, dust-like endothelial precipitates.
- Granulomatous: somewhat larger precipitates, “greasy”, partly confluent often inferiorly in Arlt’s triangle
- small stellate precipitates distributed over the entire endothelium (also granulomatous) in Fuchs’ heterochromic cyclitis
- Corneal epithelium
{kind=link}
{kind=link}
{kind=link}
- Intraocular pressure
- elevated: typically in granulomatous: HSV, VZV, Fuchs’ heterochromic cyclitis, sarcoidosis
- very high IOP in glaucomatocyclitic crisis (Posner-Schlossmann syndrome)
- low: typically in severe uveitis with inflammation of the ciliary body, e.g. in HLA-B27+ (non-granulomatous)
- elevated: typically in granulomatous: HSV, VZV, Fuchs’ heterochromic cyclitis, sarcoidosis
- Iris
- Atrophy
- Diffuse (patchy) iris transillumination: HSV, Fuchs’ heterochromic cyclitis
- Fuchs’: affected iris is usually lighter colored (=heterochromia)
- CAVE: if the iris is very bright, it can also be darker than the opposite side.
- Fuchs’: affected iris is usually lighter colored (=heterochromia)
- Sector-shaped iris transillumination: VZV
- Diffuse (patchy) iris transillumination: HSV, Fuchs’ heterochromic cyclitis
- Granulomas: nodules in granulomatous uveitis (sarcoidosis, tuberculosis, Fuchs’ heterochromic cyclitis)
- Koeppe: at pupillary margin
- Busacca: iris stroma
- Berlin: in the anterior chamber angle, typically in sarcoidosis
- Atrophy
- Lens
- posterior subcapsular cataract: heterochromic cyclitis
- Typically unilateral: Fuchs’ heterochromic cyclitis
Work-up
- In case of a mild first episode with no signs of systemic disease: no further work-up needed
- In case of a severe first manifestation or recurrent uveitis:
- Differential blood count, CRP, BSR, ANA, Syphilis, Tuberculosis, HLA-B 27, Lyme disease, ACE + Lysozyme + IL-2
- Chest X-ray / Chest CT if necessary
- Consider anterior chamber puncture (e.g. in the case of segmental iris atrophy (HSV?) or in the absence of a response to therapy).
- Consider rheumatology consult
Therapy
- Pred Forte gtt (Prednisolon) initially usually hourly (depending on anterior chamber cells) + consider additional Ultracortenol ointment (Prednisolon) at night; reduce slowly if response is good.
- Possible regimen:
Pred Forte hourly for 1 week, then two-hourly for 1 week, then 5x/d for 1 week, then 4x/d for 1 week,
then 3x/d for 1 week, then 2x/d for 1 week, then 1x/d for 1 week, then STOP
- Possible regimen:
- Scopolamine gtt 2x/d if marked anterior chamber cells (to prevent posterior synechiae)
- in case of long persistent anterior chamber cells/ pronounced inflammation:
- Consider systemic therapy with Spiricort (Prednisolon), initially 1mg/kg or subconjunctival application of Triamcinolon (Kenakort -> subconjunctivally after local anaesthesia, 10mg superior and 10mg inferior or 20mg inferior).
- CAVE: rule out infectious causes before starting therapy with systemic steroids!
Sources
- EyeWiki Acute Anterior Uveitis
- EyeWiki Treatment of Uveitis
- AAO 10 Clinical Pearls for Treating Uveitis
- Rathinam SR, Babu M. Algorithmic approach in the diagnosis of uveitis. Indian J Ophthalmol. 2013;61(6):255–262. doi:10.4103/0301-4738.114092
- Herbort CP. Appraisal, work-up and diagnosis of anterior uveitis: a practical approach. Middle East Afr J Ophthalmol. 2009;16(4):159‐167. doi:10.4103/0974-9233.58416
- Esra Guney, Ilknur Tugal-Tutkun. Symptoms and Signs of Anterior Uveitis. US Ophthalmic Review, 2013;6(1):33–7 DOI: 10.17925/USOR.2013.06.01.33
- Augenklinik Charité: Vortrag AAD 2017 Virusinfektionen des Auges, U.Pleyer, T. Lapp
- Artikel von Dr. Trevor Gray: Differentiating between Dendrites and Pseudo-dendrites: Quick-fire case presentation.
- The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease; Nika Bagheri MD, Brynn Wajda MD, et al; Lippincott Williams&Wilkins; 7th Edition (2016)
- Kanski’s Clinical Ophthalmology: A Systematic Approach; Jack J. Kanski MD, Brad Bowling MD; Saunders Ltd.; 8th Edition (2015)
- 1, 2, 3 von Eyerounds.org, © The University of Iowa; Licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License (CC BY-NC-ND)